The 14th CTAD conference returned to Boston as a hybrid meeting, reuniting colleagues long separated by COVID, while also streaming most of the scientific program to viewers around the world. The conference featured morsels of news in the effort to move anti-amyloid antibodies past imbursement barriers at the CMS, and through the approval process at the FDA, respectively. Tau antibodies mostly came up short again, and a platform trial is forming to take on this complex target more systematically. Plasma biomarkers continued their rapid advance. Digital versions of known and new cognitive tests drew note, as did AI-based projects to detect subtle changes in a person’s speech.
Aduhelm Lowers Tau; Registry to Track Real-World Performance
Despite the biomarker-based conditional approval of Biogen/Eisai’s aducanumab (trade name Aduhelm) for Alzheimer’s treatment, questions linger about how safe it is, how well it works, and whether it will improve people’s lives. Researchers addressed those issues at the Clinical Trials on Alzheimer’s Disease conference, held in Boston and online November 9-12.
Oskar Hansson of Lund University, Sweden, presented an analysis of blood samples from the Phase 3 EMERGE and ENGAGE trials. It strengthened the argument that aducanumab lowers phospho-tau, and that that correlates with cognitive benefit. Meanwhile, the Alzheimer’s Association announced the formation of a registry to gather data on the real-world effects of approved disease-modifying AD treatments, in order to judge their value to patients. Right now, that category includes only aducanumab, but other drugs in this class are expected to follow next year. Eisai/Biogen’s lecanemab and Eli Lilly’s donanemab have both started submitting data to the FDA as part of a rolling submission for accelerated approval, and Roche’s Phase 3 gantenerumab studies will read out next year.
A CTAD talk on a reasonable price for those drugs concluded that they will only be cost-effective if they go for a time-limited, not indefinite, course of treatment. For aducanumab, cost and absent insurance coverage mean fewer patients than expected are on it so far. In a new blow to aducanumab’s prospects, the European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) voted down its marketing application at a recent November meeting. A final decision from the agency is expected next month (Endpoints News). Despite this no-confidence vote for aducanumab, researchers expect clinical use of anti-amyloid antibodies to grow starting next year.
“We are at the beginning of a new treatment era,” Steve Salloway of Butler Hospital in Providence, Rhode Island, said at CTAD, noting the advent of plasma and imaging biomarkers as well as amyloid-lowering drugs. “We have the opportunity to build on this.”
Dunking Tau. Plasma p-tau181 fell in people who took aducanumab as part of the Phase 3 EMERGE (left) and ENGAGE (right) trials, with higher doses (blue) having a greater effect than low (green). In people on placebo (gray), p-tau rose. [Courtesy of Biogen.]
Effect on Tau Looks Real
One question researchers are still asking is how amyloid-lowering drugs bolster cognition, when numerous studies have shown that it is tau pathology that degrades neuronal function. Many think it is because removing plaque lessens tau pathology as well, as seen in trials of several anti-amyloid antibodies. In aducanumab’s EMERGE and ENGAGE trials, p-tau181 and total tau edged downward in the cerebrospinal fluid during treatment, as did the tau PET signal (Dec 2019 conference news). Alas, these substudies were tiny, with 131 people in the CSF and just 36 in the tau PET subgroup, leaving wide open the possibility that this was statistical noise.
To settle this, Biogen researchers had the Pennsylvania-based CRO Frontage Laboratories analyze stored plasma samples from all ENGAGE and EMERGE participants who had given blood at baseline and at completion. Because many people did not finish the trials due to the early stoppage, ARIA, or other reasons, this group amounted to a little more than half the original participants, or 1,815 people. They had given blood an average of four times each, for 6,929 total samples. Frontage Labs measured p-tau181 in these samples using a Quanterix Simoa Advantage kit. These kinds of ultra-sensitive plasma assays were not widely available when the EMERGE/ENGAGE trials were running (Apr 2018 conference news; Apr 2020 conference news).
At CTAD, Hansson presented these results. Plasma p-tau181 rose by around 9 percent in the 620 participants on placebo, reflecting worsening disease (Jan 2021 news). It fell about 15 percent in the 571 people on high-dose aducanumab, and almost as much in the 624 people on low-dose. This drop and the waning amyloid PET signal correlated, with a coefficient of about 0.4. Plasma p-tau181 dwindled the most in people whose plaque load receded to below the preset amyloid-positivity threshold of SUVR 1.1 by the end of the trial.
Notably, the drop in p-tau181 was associated with slower decline on the MMSE, CDR-SB, ADAS-Cog13, and ADCS-ADL, though it was not clear if this association was made on a per-patient or responder group level. The findings were significant, with p values typically below 0.01.
Gil Rabinovici, University of California, San Francisco, called the findings encouraging. He noted their agreement with the donanemab studies (see Part 2 of this series), where a slowing of tau tangle accumulation correlated with delayed cognitive decline (Mar 2021 conference news). “This confirms plaque clearance modifies downstream pathology,” Rabinovici said at the conference.
That said, the correlation between soluble p-tau181 and cognition was weak, with coefficients between 0.1 and 0.2. Rabinovici thinks this makes sense, because soluble p-tau is far upstream of neurodegeneration, and other factors influence the outcome along the way. Recent work from Hansson’s group suggests soluble p-tau mediates the relationship between plaques and tangles, with tangles then triggering neurodegeneration and cognitive decline (Mattsson-Carlgren et al., 2020; Mattsson-Carlgren et al., 2021). Rabinovici noted that data on how plaque removal affects neurodegeneration is sparse, and Hansson said that plasma NfL and other neurodegeneration markers are currently being assessed in the EMERGE/ENGAGE samples.
Researchers at CTAD speculated that plasma p-tau has potential as a future marker of drug response, but said the findings are too noisy to be informative at the level of an individual person. “I see the door opening for a wide application of these, but we’re not quite there yet,” said Jeffrey Cummings of the University of Nevada, Las Vegas.
A Slew of Post-Market Studies
Most new data on aducanumab will come from post-market studies, and a number of these have sprung up. Beyond the open-label extension study EMBARK and the real-world observational study ICARE, Biogen is still designing the FDA-required confirmatory trial.
At CTAD, Maria Carrillo of the Alzheimer’s Association announced a broader effort to evaluate disease-modifying AD treatments, called the National Treatment and Diagnostic Alzheimer’s Registry. Established in collaboration with the American College of Radiology, the American Society of Neuroradiology, and Brown University’s School of Public Health, the registry will enable healthcare providers to enter data on how new AD treatments affect their patients’ health and quality of life. The goal is to track how these therapies perform in the real world, and to guide policy and funding decisions, Carrillo said. Similar registries exist for other diseases, such as the National Cardiovascular Data Registry and the National Program of Cancer Registries. The association will help fund the registry’s start, and will tap personnel and administrative systems originally developed for the similar post-market IDEAS study of amyloid PET imaging (Aug 2017 conference news; Aug 2020 conference news).
As for ongoing aducanumab studies, Sharon Cohen of the Toronto Memory Program offered a first look at baseline data from EMBARK. Cohen was an ENGAGE site investigator and sits on the aducanumab steering committee. EMBARK has enrolled some 1,700 participants, roughly half the cohort from the Phase 3 trials. Almost half of them were previously on placebo; the remainder had been off drug for an average of 1.7 years when they started the extension. They also include 29 people who were already in the long-term extension of the PRIME Phase 1 study, and thus some of them have been on this drug for going on nine years. Regardless of their aducanumab history, all EMBARK participants were titrated up to a 10 mg/kg dose, and will get this monthly for two years.
EMBARK includes those who chose to come back, not a random sample from prior trials. Cohen’s data show that EMBARK’s enrollees better maintained their abilities on the CDR-SB than those who did not come back; in other words, the healthiest returned for EMBARK. Nonetheless, they had more advanced disease at baseline than the original Phase 3 cohort did, as would be expected. Their average MMSE was 21, compared to 26 in EMERGE and ENGAGE at baseline, and they were almost five years past an AD diagnosis on average, as compared to one year at EMERGE and ENGAGE. There, 80 percent of participants started out with mild cognitive impairment, 20 percent with mild AD. At EMBARK baseline, 30 percent had MCI, 42 percent mild, 23 percent moderate, and 4 percent severe AD dementia.
What happened to their cognition during the period between? People who had been on aducanumab worsened at the same rate during the gap as those who had been on placebo, but they maintained the numerical advantage they had gained on the CDR-SB, MMSE, and ADAS-Cog13, Cohen reported. This is generally interpreted as a sign that disease progression was slowed while on drug. With symptomatic treatments, cognition worsens to control levels once the drug is withdrawn. The same pattern of sustained benefit was seen with lecanemab during treatment gaps (see upcoming story).
Only 155 of the EMBARK participants got amyloid scans, as had been the case in EMERGE and ENGAGE. Their PET signals remained low throughout the gap, showing that once plaque is gone, it stays gone for this time period. This matches previously shown findings from lecanemab and donanemab (Dec 2019 conference news; Aug 2021 conference news; Aug 2021 conference news).
Hairy Eyeball On ARIA
Aducanumab is currently dogged by the question of how safe it will be in the general population, given the rates of ARIA seen even under trial conditions with rigorous safety protocols and the exclusion of cardiovascular disease (Oct 2021 news). The potential risk means patients need close monitoring via MRI. The Appropriate Use Recommendations AD leaders developed offer guidelines for when to scan, but do not specify the technical protocol (Aug 2021 conference news).
At CTAD, Tammie Benzinger of Washington University in St. Louis described an effort to do just that. Working with imaging experts around the world, Benzinger developed a standard MRI protocol to be used at all ICARE sites in the United States. There are about 200 such sites at the moment, which enroll patients who were prescribed aducanumab by their doctor (Aug 2021 news).
The standard protocol will require 20 minutes in the scanner, and calls for four scans. A 3D fluid-attenuated inversion recovery (FLAIR) scan, which suppresses CSF artifacts and is highly sensitive for detecting lesions, should be used to monitor for the edema known as ARIA-E (for review see Naganawa, 2015). To detect the microhemorrhages of ARIA-H, researchers should use a T2*-weighted gradient-recalled echo (GRE), which can detect iron deposits (Tang et al., 2014). Also part of the set is diffusion-weighted imaging, which detects ischemic strokes that can mimic the effects of ARIA, aiding differential diagnosis (Baliyan et al., 2016). Finally, the protocol calls for a 3D T1-weighted gradient echo (GE), a structural scan that will help assess brain atrophy and disease progression.
The 3D FLAIR and 3D T1-weighted GE will use the protocol from ADNI 3, while the T2*-weighted GRE will use that from EMERGE/ENGAGE. Parameters will be specified for both 3T and 1.5T scanners, Benzinger said. The protocol will be disseminated through conference talks, publications, physician groups, and scanner manufacturers. Having a standard protocol will help ICARE estimate the incidence of ARIA, track health outcomes, and compare adverse events in ARIA versus non-ARIA groups, Benzinger noted.
Such data are needed because ARIA continues to be a worry. In a poster at CTAD, Stanford University’s Sharon Sha described the case of an APOE4 carrier in Biogen’s Phase 1 PRIME long-term extension study who developed ARIA on six separate occasions over the course of nearly four years on drug. All six instances were asymptomatic and resolved after dosing was lowered or suspended. As a result of these treatment interruptions, the participant never received sustained dosing at the maximum 10 mg/kg, but did dip below the amyloid positivity threshold after 21 total doses, Sha reported (Hall et al., 2021). This case shows that ARIA can make multiple appearances even after years on drug, raising the question of how long patients need MRI monitoring.
More ominously, the FDA is investigating the death of a 75-year-old woman outside the U.S. who received aducanumab as part of the global EMBARK study. She was hospitalized and there, ARIA-E was seen on a brain scan. The case is logged in the FDA’s Adverse Event Reporting System (FAERS). An analyst who reviewed the case report, Brian Abrahams at RBC Capital Markets, believes her death was likely precipitated by epileptic seizures brought on by ARIA; Biogen states the case may be more complicated (Endpoints News). FAERS also contains six new reports of adverse events in U.S. patients on aducanumab, two of them seizures. Around 200 people are believed to have received the drug since June. Speaking off the record, a half-dozen clinicians at CTAD said they worry that all anti-amyloid antibody companies may be less than transparent about the extent and severity of ARIA they see.
Is Aduhelm Worth the Cost?
Perhaps the most roundly criticized aspect of this new drug is its price tag, $56,000 per year. At CTAD, Eric Ross of Massachusetts General Hospital, Boston, took a look at what pricing might be reasonable for anti-amyloid antibodies. He used data from aducanumab and donanemab, the latter of which is unique among current antibodies in requiring only a limited course of treatment (Mar 2021 conference news). Donanemab does not yet have a price, so Ross set a hypothetical one of $56,000 to directly compare it to aducanumab. To assess the value of these new treatments, Ross calculated their incremental cost-effectiveness ratio (ICER—not to be confused with the institute of the same name, see below) in relation to acetylcholinesterase inhibitors and memantine, the current standard of care for AD. A new treatment is usually considered cost-effective if it costs less than $150,000 per quality-adjusted life year (QALY) gained over existing treatments.
Alas, at an annual price of $56,000, both aducanumab and donanemab fell far short of that goal, with the former costing $1.8 million per QALY, the latter $300,000. The main reason for the difference was the time-limited nature of donanemab treatment. Donanemab dosing stops at a preset amyloid level, which half of Phase 2 trial participants reached within one year. For context, treatment with a rivastigmine transdermal patch, a currently available AD therapy, has a cost-effectiveness ratio of $93,000 per QALY when compared to donepezil pills (Yunusa et al., 2021).
Aducanumab would become cost-effective at an annual price of $3,000, as calculated with EMERGE/ENGAGE efficacy data presented so far, Ross said. These data have not been published in a peer-reviewed journal yet. Using a more optimistic efficacy estimate derived from Biogen’s post hoc analysis of these trials, the annual price could be as much as $11,000. These estimates are near the $3,000-8,000 range suggested as a fair price by the Institute for Clinical and Economic Review (Aug 2021 conference news). Donanemab would be cost-effective at an annual price of $20,000 or less, due to its higher reported efficacy and shorter time course, Ross said.
“We are not at a cost-effective point yet for anti-amyloid antibodies, but we are not far away,” Ross concluded. “The treatment that will get us there will be of limited duration.”
Other anti-amyloid antibodies may debut at lower prices. Roche’s head of pharmaceuticals has hinted that his company may undercut Biogen’s price if gantenerumab is approved for clinical use (Reuters news). Society’s willingness to pay for an effective Alzheimer’s therapy could rise. A recent study noted that if non-healthcare costs and caregiver well-being are included when calculating QALYs, then a hypothetical treatment costing $192,000 per QALY could drop as low as $74,000 (Ito et al., 2021).
Aducanumab’s cost is a roadblock to its rollout (NPR news; Endpoints News). Nonetheless, the prospect of greater uptake in 2022 already has the Centers for Medicare and Medicaid Services raising Medicare premiums, and has renewed calls in some quarters to let the agency negotiate prices (Endpoints News; Boston Globe).
Clinicians at CTAD lamented the resistance of insurers and hospital systems to include aducanumab in their formularies. “I don’t think it’s reasonable for pharmacy committees to try to digest this nuanced dataset and rule on it,” Rabinovici said. “That takes the decision away from doctors. I don’t think this is good for patients, and I hope this will change.”
And aducanumab’s approval, controversy notwithstanding, means Alzheimerologists are looking ahead to upcoming trials of concurrent anti-amyloid antibody and other therapies in hopes of hitting multiple disease pathways. No one expects anti-amyloid antibodies to be able to stanch Alzheimer’s disease progression on their own. DIAN is already doing so with lecanemab and an anti-tau antibody, and others are planning such trials, as well. “Combination therapy is a necessity. Everyone is coming to that conclusion,” Ron Petersen of the Mayo Clinic in Rochester, Minnesota, said in a keynote address following his acceptance of the CTAD 2021 Lifetime Achievement Award.—Madolyn Bowman Rogers
Donanemab Phase 3 Puts Plasma p-Tau, Remote Assessments to the Test
Donanemab, a monoclonal antibody trained against Aβ plaques, is hot on the heels of its slightly more advanced competitors aducanumab (see Part 1 of this series), and lecanemab (see Part 5) in the race for regulatory approval. Neck-in-neck with them: gantenerumab (see Part 6). So what's the latest? At this year’s Clinical Trials in Alzheimer’s Disease meeting, held November 9-12 in Boston and online, scientists from Eli Lilly and their academic partners parsed results from a completed Phase 2b study, reported baseline data from an ongoing Phase 3 trial, and showcased a new, decentralized approach of their prevention trial, also in Phase 3.
Most of the discussion focused on how best to deploy tau measurements—both PET scans and blood tests—to pick out just the right participants for trials and maybe even gauge how well they will take to treatment. Scientists reported that plasma p-tau-181 works to select people likely to harbor both plaques and tau tangles in the brain, and that those who start on donanemab with few tangles benefitted the most from amyloid riddance. Donanemab slowed, but did not stop, tangle growth. In all, the findings underscored that treating earlier in the course of disease stands a better chance of curbing progression.
Donanemab targets a form of Aβ with a pyroglutamate modification on its N-terminus. Earlier data from the Phase 2 TRAILBLAZER study had shown that the antibody binds and clears its target, found only on plaques, remarkably well (see Mar 2021 conference news and Mintun et al., 2021). The trial enrolled 257 people who had an intermediate level of tau tangles as per tau PET, as well as amyloid accumulation above a threshold of presumed brain-wide abnormality set at 24 centiloids. Participants got monthly infusions of placebo or donanemab for 76 weeks, or until their amyloid levels dropped to 11 centiloids at one visit or below 24 for two consecutive scans. As reported before, 40 percent of treated people had “normal” levels of amyloid by 24 weeks, and 68 percent did by the trial’s end. Treatment slowed decline a tad, by 32 percent, on the integrated AD rating scale. The iADRS is Lilly’s customized composite of the ADAS-Cog and ADCS-iADL.
At AAIC, scientists reported that plasma p-tau-217 had edged down with treatment, and linked its reduction to slower cognitive decline. This cast this blood marker as an indicator of brain amyloid reduction and strengthened the tether between Aβ and tau in the amyloid cascade hypothesis of AD (Aug 2021 conference news).
Based on the data from its Phase 2 trial, Lilly announced late last month that it had started an FDA application for accelerated approval, which it will file by rolling submission of data as it comes in. It expects to complete this within the next few months. Lecanemab started the same process a month prior (Oct 2021 news).
At CTAD, scientists offered a deeper analysis of how amyloid and tau burden relate to treatment effect. Lilly’s Sergey Shcherbinin reported that, when used as a screening tool for the Phase 2 trial, tau PET selected not only participants with intermediate tau accumulation, but also with amyloid. After meeting the trial's cognitive criteria, people received a tau PET scan. Of those, 37 percent had an intermediate level of tangle accumulation and of those, 96.5 percent were subsequently found to have an amyloid plaque burden of at least 24 centiloids, meeting the trial's inclusion criteria.
Once enrolled, participants slid into the scanner for baseline scans, then again for more amyloid-PET scans every 24 weeks throughout the trial, and for a second tau PET scan at 76 weeks. Such serial data enabled Shcherbinin to see that the growth rate of tangle burden throughout the trial correlated with the degree of amyloid removal. Specifically, people whose amyloid burden had dropped below 24 centiloids by six months had less tau accumulation over the course of the trial than did people whose amyloid was only partially cleared by that time, although both groups benefited.
Breaking down the tau PET data regionally, Shcherbinin reported that donanemab treatment worked best at reducing tangles in various regions of the frontal lobe, which tends to get invaded after the temporal and parietal lobes have succumbed. The effect was striking in the frontal medial superior cortex, where donanemab curbed tau accumulation by nearly 100 percent in people who had cleared amyloid by 24 weeks, and by about 60 percent in people with partial early clearance.
Shcherbinin tied less tau progression in different lobes to the slowing of decline in different cognitive domains. For example, less tracer uptake in the temporal, parietal, and frontal lobes correlated with slightly better orientation, while tau reduction in the temporal and parietal lobes correlated with better word-finding. That said, none of these lobar tau measurements correlated with the global ADAS-Cog13 score.
Onward to Phase 3
Other scientists presented baseline data from the confusingly named TRAILBLAZER-2. This is a Phase 3 trial in people with early AD. Lilly's John Sims reported that, analogous to what had been done with plasma p-tau-217 in Phase 2, here the scientists adapted a plasma p-tau181 assay to the Simoa platform. Then they asked if it would work as a prescreening tool for enrollment in the Phase 3 trial.
Plasma p-tau-181 was measured among a subset of 752 potential enrollees before they had amyloid- and tau PET scans, while 3,619 other people had the PET scans without this prescreen. Among the 752, p-tau-181 predicted the presence of both amyloid and tau pathology. Sixty-three percent of those with elevated blood p-tau-181 turned out to have both plaques and tangles on PET, whereas only 37 percent harbored both types of deposit among those who got tau scans without prescreening. Sims said that in future trials, plasma pre-screening will help avoid unnecessary scans, reduce cost, and make trials accessible to people who live in regions without nearby PET centers.
Lilly’s Paul Solomon described the volunteers who are in this trial, which is fully enrolled. As of October 15, TRAILBLAZER-2 had randomized 1,625 participants. Nearly three-quarters live in the United States, the rest are in Japan, Canada, Poland, the Czech Republic, United Kingdom, The Netherlands, and Australia. It took screening more than 8,000 people to net these precious enrollees.
Solomon used this cohort's baseline data to compare demographic and disease features between people with intermediate versus high levels of tau pathology. Relative to people with intermediate tangle burden in either the Phase 2 or 3 studies, those with high tau in this new trial were younger. More of them were women, ApoE4 noncarriers, and on acetylcholinesterase inhibitors. They posted worse baseline scores on the MMSE, ADAS-Cog11, and CDR-SB, and were likelier to have mild AD than MCI. Interestingly, the baseline amyloid plaque burden between those with intermediate and high tangle burden was about the same. In all, this suggests that a person's tangle burden correlates with the stage of their clinical disease.
TRAILBLAZER-2 is designed much like the Phase 2 trial, which is typical for Phase 3 studies meant to confirm a Phase 2 efficacy signal. There is a notable difference, though, in that Lilly broadened the inclusion criteria to also include people with a lot of tau pathology, and indeed the baseline data appear to reflect a subcohort with somewhat “worse” AD.
Paul Aisen of the University of Southern California, San Diego, believes this might have been a mistake. He noted that even among people in the Phase 2 trial, which included only people whose tangle burden was intermediate, those on the higher end of this limited spectrum did not benefit from donanemab. “The data are pretty clear that the higher the baseline tau, the lower the response,” Aisen said. “It’s hard to understand the idea of broadening the inclusion criteria.”
Sims told Alzforum that including people with high tau, who tend to be younger and face a faster-progressing disease, will help future prescribers understand this population and whether they will benefit from donanemab. “Our goal for enrolling high-tau participants is to provide those answers while not jeopardizing the success of TRAILBLAZER-2,” Sims wrote. “We believe we can achieve both with our trial design, which will involve analyses that look at the intermediate tau group separately and also the total trial population.”
Separately at CTAD, several different neurologists besides Aisen questioned Lilly’s approach of stopping donanemab after amyloid scans normalize. They noted that while amyloid plaques remained at bay for some time after treatment discontinuation in Phase 2, there are indications that the disease could be picking up steam again. In the lecanemab Phase 2 trial, the blood Aβ42 to Aβ40 ratio—an indicator of amyloid accumulation—started to worsen again once participants were off that drug. “We may be relying too heavily on amyloid-PET, which is perhaps a slow responder to the effects of discontinuation,” Aisen said.
However, at CTAD, Sims made the case that plasma p-tau-217 stays low—for a year, at least—after donanemab treatment stops. Splitting the Phase 2 treatment groups into those who had cleared amyloid by 24 weeks and thus were moved to placebo at that time, and those who hadn’t, Sims reported that p-tau-217 stayed low until the end of the trial in both groups.
Go Down Stay Down? Plasma p-tau217 dropped in response to treatment with donanemab, and stayed low even among participants who stopped treatment at 24 weeks. [Courtesy of Eli Lilly & Co.]
Sims also noted that previous modeling studies suggest that following amyloid removal with donanemab, it would take three to four years for participants to return to amyloid-positive levels, and up to 14 years to return to their baseline plaque load. “It is important to test the hypothesis that once a pathology is removed that patients do not need to be subjected to continual therapy,” Sims wrote.
While TRAILBLAZER-2 expanded to fold in those with worse pathology, a third trial, TRAILBLAZER-3, is moving in the other direction. This secondary prevention trial—run with the Banner Alzheimer’s Institute in Phoenix—has started inviting people with amyloid accumulation but no clinical symptoms. At CTAD, Banner’s Pierre Tariot detailed its rationale and design.
Starting out with iADRS scores from donanemab's Phase 2 trial, split into tertiles of baseline tau PET, Tariot said those with the least tangles at baseline had benefited the most from treatment. Although everyone in this trial was already symptomatic, Tariot believes the data argue for treating people before they have tangles.
TRAILBLAZER-3 targets people in the preclinical stage, when amyloid is accumulating but symptoms have yet to surface. How to find such people is perhaps the field's most pressing question these days. For this trial, Lilly and Banner are using several tools to draw in potential participants. For one, they are tapping the Alzheimer’s Prevention Registry’s initiative, which has assembled 364,000 registrants. They are also bringing in recruits via clinicians across the United States who know interested patients, and through Lilly outreach efforts to community organizations, health centers, and pharmacies.
Candidates for the trial go through a screening process that does not require a single person to set foot inside a centralized study site, Tariot said. Rather, the trial embraced a new, decentralized design that relies on plasma biomarkers and remote assessments.
Recruits must be between 55 and 80 years old. They will be screened for lack of cognitive impairment via the modified telephone interview for cognitive status (TICS-m), a 13-item cognitive test that can detect amnestic mild cognitive impairment (Cook et al., 2009). These calls are made with centralized raters contracted by Lilly. Then, in a first for the field, plasma p-tau217 levels are used to screen for elevated brain amyloid in those who were deemed to be cognitively normal over the phone. Candidates can get their blood drawn for this test at designated sites near where they live, such as Quest Diagnostics. Those with elevated plasma p-tau217 complete the consent and enrollment process via video calls. Yes, that's all.
Once they are in, participants take their donanemab or placebo infusions at local, certified infusion centers. They will receive brain MRIs at baseline and two more times over the first five months of the trial, or as needed if concerning symptoms, such as those suggesting ARIA, emerge. Participants can get these scans at any certified MRI center. Tariot said there are few parts of the country without one, as MRI is more widely available than PET.
Blazing a Decentralized Trail? Most participants will never set foot inside a trial site. They receive infusions, blood draws, and MRIs at nearby locations, and take cognitive assessments via video call. A central study coordinator ushers them through the process, and a principal investigator oversees safety. [Courtesy of Eli Lilly.]
'Homework,' But No Appointments at the Clinic
Cognitive and neuropsychological assessments are going to be remote, Tariot said. Each participant will be assigned two central raters—one who will conduct the CDR-SB interview, and another who will conduct an array of other psychometric assessments, including the International Shopping List Test, Continuous Paired Associate Learning, Cognitive Function Index, and the Montreal Cognitive Assessment, which will serve as secondary outcomes. Both sessions happen every six months via video call. In addition to these raters, each participant gets a study coordinator who will usher them though the process of each assessment. Besides the rater-based assessments, participants will take several self-administered tests on study-issued tablets, which come with a hot spot to boost internet connectivity, if needed. Principal investigators are to oversee safety concerns of all participants within a given region.
The only time people may need to travel to a specialized center is for amyloid- or tau PET scans. Tariot said that the established sensitivity of plasma biomarkers has made this optional for participants. The trial aims to collect florbetapir-PET data on 200 people and flortaucipir-PET scans on 500 people. These participants are likelier to live in major cities where PET is available.
Hopefully, this approach will remove barriers to trial participation and speed up enrollment, Tariot said. Lilly and Banner are aiming for 3,300 participants. Enrollment is going smoothly, Tariot said, but he would not say how many people have joined, or how long he estimates filling the trial will take.
Hello Again, Time-to-Event?
While TRAILBLAZER-3 exemplifies a new design, its primary endpoint—time to emergence of cognitive impairment—harkens back to the early days of AD trials. Participants are randomized 1:1 to receive nine monthly infusions of placebo or donanemab. After that, infusions end and participants will be monitored every six months on their global CDR-SB, which tallies up impairment in six domains with memory considered the primary. This will continue until 434 participants have become cognitively impaired, i.e., scored above zero on the global CDR for two consecutive visits. Called 'time to progression to aMCI, this will be the trial's primary endpoint. Tariot said the groups' modeling predicts this will happen three years after enrollment is complete. The hope, clearly, is that those who progressed will have been on placebo.
After the trial's blinded portion ends, those who were on placebo can opt to receive nine doses of donanemab in the open-label extension. There are no plans to give another series of infusions to the original treatment group.
The trial's return to a time-to-event primary endpoint sparked debate. This used to be the norm in the field's early trials, but since has been discarded in favor of continuous measures. At CTAD, Michael Weiner of the University of California, San Francisco, questioned the choice. Previous studies had found that endpoints that incorporate changes in the rate of progression over time have more statistical power than those comparing singular events such as progression to MCI (Li et al., 2019). Aisen made a similar point, noting that the disease's gradual progression means discrete stages, and the binary decisions they require, are artificial. “When you separate disease progression into discrete stages to make a time-to-event design, you are throwing away the majority of the information as well as statistical power,” he told Alzforum.
Sims countered that Lilly is looking for a result that matters to people. “Nothing could be more meaningful than preventing progression to MCI,” he said. If disease is truly progressing over time in this preclinical population, then this endpoint should be able to detect a meaningful difference between treatment and placebo groups. Tariot told Alzforum that extensive mathematical modeling strongly suggested that the time-to-event endpoint was likeliest to detect a treatment effect in this study. This would imply that in those earlier time-to-event trials that were negative, the problems had been the drugs and insufficiently specific inclusion criteria, more than the endpoint.
But wait, there’s more. Lilly has plans for a third Phase 3 trial—TRAILBLAZER-4. It will compare the plaque-clearing prowess of donanemab to that of aducanumab head-to-head in 200 people with mild AD. That trial, which will use biomarkers of amyloid clearance as endpoints, is slated to start enrolling later this year.—Jessica Shugart
Plasma Aβ—First Sign of AD, But Tough to Measure Prospectively?
Scientists believe that poor clearance of Aβ from the brain underlies sporadic Alzheimer’s disease. Now, evidence for subtle changes in the plasma levels of Aβ1-42 seems to back that up. At this year’s Clinical Trials in Alzheimer’s Disease meeting, held November 9-12 in Boston and online, scientists led by Suzanne Schindler, Washington University, St. Louis, reported that the plasma Aβ42/40 ratio not only falls in people at the very earliest stage of the disease, it does so years before that ratio drops in the CSF.
Schindler’s tantalizing hypothesis is that at the point of origin of AD, the plasma Aβ42/40 ratio begins to fall not because Aβ42 peptide has begun to form plaques in the brain—the generally accepted hypothesis—but because less of it seeps out of the brain as people age. Only later does the peptide form plaques and soak up peptide that would otherwise show up in the CSF. If true, this nuanced view would peg plasma Aβ42/40 ratio as the very first marker to change in AD. This could have implications for the basic understanding of Alzheimer’s pathophysiology and potentially the way it is treated.
It could also support using the plasma Aβ42/40 ratio for screening in trials that aim to nip the disease in the bud. Alas, for that, this measure may be finicky. Data presented by Christina Rabe, Genentech, South San Francisco, threw cold water on the screening idea. She reported that because the plasma Aβ42/40 change is so subtle, any small bias or variance in measurements or pre-analysitical handling would generate such high false positive and negative calls that trial candidates could end up being misclassified. Others pushed back, claiming that highly accurate tests and good quality control can make the measure robust enough for screening in trials, and even for general diagnostic use. The Alzheimer's Clinical Trials Consortium's AHEAD 3-45 trial of lecanemab has already begun to use C2N’s CLIA-approved mass spectrometry test for plasma Aβ to prescreen volunteers before running amyloid PET scans.
Plasma First
Schindler’s analysis was based on the large dataset from the Knight ADRC at WashU of people who have been volunteering for the center's multiple, decades-long observation studies. First, she determined how well C2N’s test, called Precivity, captured amyloid positivity as judged by either CSF Aβ42/40 analysis or PET scans.
Among 1,085 volunteers who'd had lumbar punctures and 710 who'd had PET scans, Precivity scores correctly predicted amyloid status by either measure with an area under the curve (AUC, a statistical measure) of 90 percent accuracy. The test performed equally well in people who were cognitively normal and in those who were impaired. Schindler had reported on a subset of 158 of these people previously (Schindler et al., 2019; Aug 2019 news).
How would the test predict future amyloid status? Here’s where things got interesting. Schindler tracked 273 people who had initially tested negative for amyloid based on their CSF Aβ42/40 ratio. Curiously, about 40 of them had Precivity scores above the cutoff, i.e., were predicted to have brain amyloid plaques at that time. Were these false positives? Probably not. Over the seven subsequent years, the CSF Aβ42/40 ratio for most of these volunteers slowly sunk downward, such that their CSF now tests positive, or close to positive, as well. “This suggests to us that these were not false positives at all,” Schindler told Alzforum (see image below).
Plasma Before CSF. Among people who had tested negative (top, blue and purple dots) or borderline (green dots) for brain amyloid based on a CSF Aβ42/40 cutoff (horizontal dashed line) at baseline, those who had tested positive by Precivity cutoff (vertical dashed line) at baseline (upper right quadrant, top), were likelier to test positive by CSF seven years later. [Movie courtesy Suzanne Schindler, WashU.]
The data imply that the plasma Aβ42/40 ratio starts falling years before it does in the CSF. “This was surprising, because it is generally believed that changes in CSF Aβ are the earliest signs of AD,” Schindler told Alzforum.
Henrik Zetterberg, University of Gothenburg, Sweden, considers this data “super interesting.” He has some questions, too. “If Aβ shifts from the CSF into plaques, then how would that be visible sooner in the blood than the CSF?” he wondered. In fact, Schindler said plasma and CSF diverge before plaques begin to form. She thinks the Aβ42/40 ratio in the plasma drops because clearance of Aβ42 from the brain begins to wane even while CSF Aβ remains high.
Her data support this idea. She measured Aβ42 and Aβ40 levels in the CSF and plasma of 124 people in the ADRC cohort that was collected halfway through the seven-year follow-up. All still had high CSF Aβ42/40, indicating they were negative for amyloid in the brain. Intriguingly, when she looked at the rate of change in these volunteers, the CSF ratio was stable, but the plasma ratio had already begun to decrease. Looking at each peptide individually, she found that both Aβ42 and Aβ40 had increased in the CSF with age, meaning the ratio stayed the same. In the plasma, however, Aβ40 increased more with age than did Aβ42, suggesting that Aβ42 was being cleared less efficiently from the brain. “Plasma Aβ may be taking us back to the real genesis of Alzheimer’s, which is reduced clearance of Aβ42 from the brain,” Schindler proposed.
Prior data from Randall Bateman’s lab at WashU supports this idea. He found that Aβ is directly transported across the blood-brain barrier in people, and that this clearance slows by two- to fourfold as people age into their 70’s (Roberts et al., 2014; Patterson et al., 2015).
Kaj Blennow, also from U Gothenburg, was cautious. “If there was a drop in clearance, then why would it not be a drop for both Aβ42 and Aβ40?” he asked. He said more studies are needed to confirm what is going on. Zetterberg said this could easily be done, noting “There has been prior data suggesting that Aβ ticks up slightly in the CSF before plaques begin to form, and that would be in keeping with Schindler’s hypothesis.”
Exactly what might crimp Aβ42 clearance before plaques are even there to mop it up remains to be seen, but Schindler thinks what she found is no exception. “The interesting thing is that this seems to be happening [in the ADRC cohort], even those with high CSF Aβ42/40,” she said (see image below). Schindler and Bateman now believe that AD doesn’t necessarily start when plaques begin to deposit, but when clearance of Aβ42 begins to wane, setting the stage for incorporation of the peptide into plaques.
Clearance may be a function of age and other factors, including APOE genotype. “We would predict that we might not see the plasma Aβ42/40 ratio dropping in younger people,” Schindler said. People in the ADRC cohort ranged from age 59 to 79.
Prospective Measures
If a person's plasma Aβ42/40 ratio opens a window into AD a few years before CSF Aβ42/40, then it would be the earliest marker of AD pathophysiology. Does that also make it the best screening marker for clinical trials or suitable for diagnosis? This is the idea Rabe challenged at CTAD.
Working with Tobias Bittner at Hoffmann-La Roche, Basel, Switzerland, OskarHansson at Lund University, Sweden, Zetterberg, Blennow and others, Rabe evaluated how well the plasma Aβ ratio works as a screening tool and how robust the measure might be in a prospective setting. All these authors are stakeholders in different plasma tests for Aβ and for various forms of phospho-tau.
Plummet in Plasma. Change in plasma Aβ42/40 over a period of up to 15 years. Each line represents repeat samples taken from one of 362 people in the ADRC cohort. The black line represents their baseline measure and each dot represents a different sample collection. Colors reflect the spectrum of baseline CSF Aβ42/40 values, with purple being the highest and red lowest. Arrowheads denote the last plasma sample and show that the ratio is falling in almost all participants, regardless of their initial CSF ratio. [Courtesy Suzanne Schindler, WashU.]
To date, many labs have tested the marker and found that it can distinguish people with AD from controls and from people with other diseases with remarkable accuracy, but most of those studies were done retrospectively, by analyzing a whole collection of samples together in one fell swoop, with the same batch of reagents (Aug 2018 news). Because the ratio changes by only 10-15 percent when a person develops amyloid pathology, clinical chemists doubt the plasma Aβ ratio is robust enough to use prospectively, on a day-to-day basis for diagnostic or screening purposes. In those settings, a person comes in, gets blood drawn, has it analyzed, and the doctor makes a call about whether he or she has brain amyloid or not. For that to work for a large trial, for example, the test needs to be perfectly stable over the course of a year or so while it enrolls.
Rabe modeled the idea of prescreening for a trial in data from the Swedish BioFinder study and from ADNI, using her company's Elecsys test. First, she asked if a plasma Aβ42/40 cut-off could be found that could work as a screening tool. The issue here is not only that the ratio changes very slightly in people who have brain amyloid, but also that there is considerable overlap between the “positives” and “negatives.” Rabe found that in BioFinder, where the AD prevalence is about 15 percent, a cutoff of 0.13 would rule out 45 percent of amyloid-negatives, while only eliminating 2 percent of those who were amyloid-positive (see image below). That would cut the number of PET scans needed to recruit amyloid-positive people into a trial by about 40 percent, Rabe said—a cost savings.
Ruled Out. In this model, use of a carefully selected plasma Aβ42/40 cutoff (vertical line) could avoid negative PET scans for a majority of amyloid-negative people, enriching trial populations for people who are amyloid-positive. [Courtesy of Christina Rabe, Genentech.]
But that calculation is based on retrospective analyses—a whole batch of BioFinder samples analyzed together. Would it work one-by-one going forward? Here, Rabe was concerned about how a plasma Aβ biomarker tolerates any variance in pre-analytical sample handling, or slight batch-to-batch changes in reagents that might creep in over time and skew the results.
The large overlap between amyloid-positives and -negatives and the narrow dynamic range in this assay means that a 10 percent bias could end up shifting a large proportion of the people above or below the selected cutoff, misclassifying them (see image below). A similar bias in CSF Aβ42/40 or plasma p-tau/Aβ42 would misclassify far fewer people.
Darned Drift. With plasma Aβ42/40 measurement, any slight variation due to assay bias or sample handling could misclassify people whose result lies near the cutoff (top line). For CSF Aβ42/40 and p-tau ratios, variability has less dramatic effects because the fold change between positivity and negativity is larger. (Amyloid PET positive: blue; negative: red). [Courtesy of Christina Rabe.]
Does this matter? Rabe thinks yes. “Assay conditions will never be perfect and a small bias or random variability should not result in a reclassification of patients,” she said. Bittner told Alzforum that the crux of the matter is how much error an assay can tolerate and still perform. “We see for Aβ42/40 that there is very little wiggle room for bias or variability, which would render the assay useless,” he said. “In fact, it can be so bad that you select the wrong people and deselect the right people.”
Bittner said he was taken aback when he first saw this. “We had a hard time believing the assay was not performing prospectively. We thought it was just a problem with our Elecsys system, but when we saw data for head-to-head comparisons on the ADNI site we realized that the dynamic range is no better for any of the other assays.”
Does this issue rule out plasma Aβ42/40 as a screening marker? The risk is great that it will not work, said Blennow. As he sees it, the problem is not the technique, but the marker itself. “The fold change is so small, the groups are very close together, and you put the cutoff right in the middle,” he said. Bittner agrees, saying “Our message is that it will not work prospectively, at least over the long term. It might be good for a few weeks or months, but once bias is introduced, performance will suffer.”
Bittner said the maximum bias a plasma Aβ42/40 assay could tolerate would be 3 percent. This is near the precision of mass spec assays used in Bateman’s lab at WashU and at C2N Diagnostics, which have the only CLIA-approved plasma Aβ42/40 test. Bateman was a co-founder of C2N. These assays outperform, in retrospective analyses, immunoassay-based methods and other mass spec assays, including the ones used by Roche and the U Gothenburg team (Oct 2021 news).
Joel Braunstein, C2N Diagnostics, insists plasma markers can be measured with great precision and that C2N's mass spec assay is robust. Precivity is the company's first commercial product. Braunstein told Alzforum that C2N has not modified its cut point since they rolled out the CLIA-approved test last year. “As part of our ongoing QC, we watch for it and evaluate the appropriateness of the cut point. To date, we have never seen evidence that we should modify it. Our experience is that we can absolutely distinguish individuals with and without disease and use it in a manner that would clearly provide value in prospective trials an even in clinical use,” he said.
The argument is more than academic. The AHEAD 3 and AHEAD 45 trials have begun to use this marker. Both trials are targeting cognitively normal people who are in the earliest stages of AD and are as young as 55 (Nov 2020 news). A3 enrolls people who fall between 20 and 40 centiloids on amyloid PET, while A45 targets those above 40 centiloids. At CTAD, Reisa Sperling, Brigham and Women’s Hospital, Boston, showed that AHEAD, which started screening in the middle of the COVID pandemic, soon noticed that the screen failure rate by amyloid PET was quite high, especially among those younger than 65. To bring that down, the investigators turned to C2N’s assay, hoping to enrich for people who are likely to be amyloid-positive.
As of October 18, AHEAD had screened 659 people for plasma Aβ42/40 in a retrospective batch. Everyone had also had an amyloid scan with the NAV4694 tracer. Sperling reported that those whose amyloid PET was above 20 centiloids had lower plasma Aβ42/40 ratios, suggesting that a cutoff strategy would work in this cohort. The plasma test also picked up most of the A3 participants, who fell into the 20-40 centiloid range (see image below).
Fit for Prescreen? In AHEAD 3-45 trials, the Precivity test identified most people who tested positive for amyloid on PET. [Courtesy of Reisa Sperling.]
What about the test's robustness for prospective use? AHEAD investigator Paul Aisen, University of Southern California, San Diego, acknowledged the concern. He told Alzforum that AHEAD will re-evaluate the plasma Aβ42/40 cutoff point in these cohorts as the trial proceeds. “Because our process allows us to look at the relation of the cut-point to diversity of the population, the number of false negatives, as well as the screen fail rate on PET, there are a number of measures of the efficiency of the screening process that we will consider as the trial moves forward.” In her talk, Sperling said that AHEAD will initially err on the side of sensitivity to ensure that it misses neither potential A3 participants, who would be expected to have a smaller drop in the Aβ42/40 ratio, nor people from diverse backgrounds.
Zetterberg thinks this iterative process may take care of variability or bias that might creep into the test over time. “This approach could work, but it’s not the way clinical labs normally conduct assays, and it may be very demanding,” he said, adding that this would not be feasible if the test was to be rolled out as a routine diagnostic.
Jeffrey Dage, Indiana University School of Medicine, Indianapolis, believes a plasma Aβ assay can work. “This is an analytical and statistically heavy issue,” he wrote to Alzforum. “Robust and reliable plasma Aβ42/40 measurements need to be very high precision and the assay has to be kept in control.” Still, he believes plasma Aβ42/40 has potential for use in screening for clinical trials. “I am confident that it can work for trial enrichment and improve efficiency for preclinical AD studies, but it needs to be implemented carefully and managed closely,” he wrote. In his talk at CTAD he noted that the crux of the matter is effect size. “It’s really too small to use on its own for patient selection,” he said, but he thinks it could be used to enrich a population for a clinical trial.
Is this debate moot if those selected people are going to be scanned for brain amyloid anyway? Not if the people who are screened out after giving blood are not followed up. “We’ll never know what we missed in those who were excluded,” said Zetterberg.—Tom Fagan
Roberts KF, Elbert DL, Kasten TP, Patterson BW, Sigurdson WC, Connors RE, Ovod V, Munsell LY, Mawuenyega KG, Miller-Thomas MM, Moran CJ, Cross DT 3rd, Derdeyn CP, Bateman RJ.
Amyloid-β efflux from the central nervous system into the plasma.
Ann Neurol. 2014 Dec;76(6):837-44. Epub 2014 Oct 24
PubMed.
More Tau Antibodies Bid Adieu; Semorinemab Keeps Foot in Door
As Aβ-targeted therapeutic antibodies set their sights on regulatory approval, tau-targeted antibodies still toil near the starting line of clinical development, while some have fallen by the wayside already. At the Clinical Trials on Alzheimer’s Disease meeting, held November 9-12 in Boston, researchers debated a lone positive sign—a slowing of decline on one cognitive battery in the Phase 2 semorinemab trial—and presented the results of two failed trials. Save for that, no antibodies directed against tau’s N-terminus have benefited trial participants with AD or other tauopathies, and one, gosuranemab, may have made things worse.
Adam Boxer, University of California, San Francisco, said he is undeterred, because while anti-Aβ drugs have been tested for decades, it is early days for tau, a big, complex protein. Different ways of taking shots at tau are only beginning to come into their own. Scientists are learning which of tau’s many forms to target, in which diseases they are active, and when. As a new crop of antibodies aimed at tau’s midsection enters the fray, Boxer is hoping to build a tau platform trial that can test different tau drugs by themselves or in combination with amyloid drugs. The emergence of a clinical effect for four separate anti-Aβ therapies and the arrival of informative plasma biomarkers make for exciting days in AD clinical trials, Boxer believes. “Even though we haven’t seen a clear benefit of a tau therapy, progress is being made, and we shouldn’t give up,” he said.
Semorinemab: Blip, or Beginning of a Benefit?
At CTAD, Cecilia Monteiro of Genentech presented top-line data from LAURIET, a Phase 2 trial of semorinemab in people with mild to moderate AD. Alzforum covered the upshot when Genentech and co-sponsor AC Immune announced it (Sep 2021 news). LAURIET enrolled 272 people with brain amyloid whose MMSE scores were between 16 and 21, then randomized them to monthly infusions of placebo or semorinemab for 48 weeks. A subset who had to skip infusions due to the pandemic stuck with the trial for an additional 12 weeks. As announced previously by Genentech and AC Immune, semorinemab slowed decline on the ADAS-Cog11, one of two primary endpoints, by 42 percent at week 49 of the trial. At CTAD, Monteiro presented the data, which showed a crack open up between semorinemab and placebo groups at 25 weeks, hold steady at 37 weeks, and widen by 49 weeks, at which point the semorinemab group appeared stable. This benefit was driven primarily by the memory domain of the composite test, Monteiro said.
Noise, or Real Effect? In people with mild to moderate AD who received semorinemab, decline on the ADAS-Cog11 slowed, especially during the final 12 weeks of the LAURIET trial. [Courtesy of Genentech.]
This was LAURIET’s lone positive result. Monteiro reported no difference between groups for the trial’s co-primary endpoint, the Alzheimer’s Disease Cooperative Study-Activities of Daily Living (ADCS-ADL), a measure of functional decline. Semorinemab did not budge scores on the MMSE or the CDR-SB, either. It had no effect on tangle accumulation as measured by uptake of Genentech's GTP1 tau tracer on PET scans.
In a panel discussion, chaired by Rachelle Doody of Roche/Genentech, clinicians attempted to make sense of this. What might be the reason for an effect on the ADAS-Cog11, but not other cognitive or functional measures, Doody asked Stephen Salloway of Brown University in Providence, Rhode Island, a site investigator for LAURIET. “When we get a single result like this, we have to be concerned about the reliability of the finding,” Salloway responded. This is especially true given the negative result of the TAURIEL trial of semorinemab in prodromal to mild AD. Urging further study, Salloway cautioned that even if the ADAS-Cog11 benefit is reproducible, it alone would not constitute a meaningful benefit at this stage of AD. Semorinemab would have to do more.
Randall Bateman, Washington University, St. Louis, is not convinced either. He noted that lack of benefit on the CDR-SB and MMSE, which also contain memory components, imply the ADAS-Cog effect may not be robust. “Patients at this stage need an impact on function, not just cognition,” he added. He thinks the most useful data will come from the ongoing open-label extension trial of semorinemab in people with mild to moderate AD. "Once the cognitive and clinical durability is known, then the robustness of the effect can better be determined," he said.
To the eyes of Gil Rabinovici, University of California, San Francisco, the leveling off of the ADAS-Cog11 decline in the treatment group in the final weeks of the trial looked unusual. Alireza Atri of Banner Sun Health Research Institute in Phoenix said that it’s possible the ADAS-Cog11 benefits appeared slowly, and CDR-SB and ADCS-ADL might show change only later. Monteiro said the ongoing open-label extension will at least show whether the ADAS-Cog11 is durable or a blip, and whether functional benefits, which tend to follow cognitive ones, might still emerge.
“While it is always exciting to see a positive result on a clinical outcome in an AD drug trial, replication will be essential for determining the robustness of the semorinemab effect on cognition observed in the LAURIET trial,” Rabinovici wrote in a comment to Alzforum. “The lack of consistency between the clinical (ADAS-Cog11) and functional (ADCS-ADL) outcomes in the trial, as well as the lack of a signal for slowing of tau spread by PET, do not paint a picture that is clearly indicative of disease slowing.”
Like semorinemab, gosuranemab binds tau's N-terminus, but unlike semorinemab, it appears to hasten decline on the same test battery. Biogen shelved gosuranemab after it failed to curb decline in progressive nuclear palsy and in early AD (Jun 2021 news). At CTAD, Biogen’s Melanie Shulman showed the top-line results of the latter study. It had enrolled 654 people who had early AD and evidence of amyloid for monthly infusions of placebo, or low, medium, or high doses of the drug over 18 months.
As reported, the trial missed its primary endpoint of change on the CDR-SB and conferred no benefit on any exploratory measure, including the ADAS-Cog13, ADCS-ADL, MMSE, and the Functional Assessment Questionnaire (FAQ). While this was expected, one result came as a surprise. All three gosuranemab dose groups declined more on the ADAS-Cog13 than placebo. A gap between the treatment and placebo groups opened at 12 months and widened by 18 months. The effect was not dose-dependent, Shulman reported, but only the highest dose group had a statistically significant difference from placebo on ADAS-Cog13 change by 18 months.
Gosuranemab bound its target, dramatically lowering N-terminal tau in the cerebrospinal fluid at all doses. Still, it did not budge tangles as per tau PET.
How might two N-terminal antibodies exert opposite effects? Afterall, both latch onto similar tau epitopes and are of the same IgG4 antibody ilk. While the answer is unknown, one difference between the two trials is the degree of impairment of enrolled participants. While semorinemab was given to people with mild to moderate AD in the LAURIET trial, gosuranemab flowed into participants with early AD. Notably, semorinemab had previously failed in people with early AD as well, though it did not make people worse. Boxer and other scientists suspect that different forms of tau may have different effects at different stages of the disease and that the N-terminal species targeted by these antibodies may only wreak havoc later on. Boxer noted that studies from Lennart Mucke’s lab at UCSF suggest extracellular tau messes with synaptic firing. Perhaps this effect differs by disease stage, and electrophysiological recordings such as EEG or MEG could possibly monitor that in future trials, he said.
Tilavonemab, also directed against N-terminal tau, sang its swan song at CTAD also. Hana Florian of AbbVie reported data from a Phase 2 trial in 453 people with early AD who had evidence of amyloid. They, too, received monthly infusions of placebo or one of three doses of tilavonemab for two years. The drug did nothing to CDR-SB scores—the primary endpoint—which worsened similarly between groups throughout the trial. Ditto for all cognitive and functional measures, including the ADAS-Cog14, RBANS, MMSE, FAQ, and ADCS-ADL. Tilavonemab curbed neither brain atrophy nor plasma neurofilament light (NfL), suggesting it did nothing to assuage neurodegeneration. Like semorinemab and gosuranemab, tilavonemab was safe and well-tolerated. AbbVie has canned tilavonemab, which had also flopped in a PSP trial (Jul 2019 news).
With the exception of semorinemab, which clings by a thread to a single signal, all tau antibodies thus far have come up short. They engaged their target in CSF and even in brain autopsy studies, but did not budge tangle accumulation as gauged by tau PET. What gives? Maybe the antibodies target the wrong form of tau, one that is not involved in the downstream formation of aggregates, Boxer said. In support of this idea, previous studies led by Bateman found that in the AD brain, N-terminal forms of tau are secreted, while full-length tau remains inside the cell (Mar 2018 news). If antibodies are latching onto these fragments, they may be doing little to halt the aggregation of tau inside cells.
It could also be that tau progression is not driven by transcellular spread of tau, which these antibodies aim to intercept. In keeping with this idea, a recent kinetics study concluded that after Braak stage III, the lion’s share of tau accumulation occurs via local replication, as opposed to dissemination from one region to another (Nov 2021 news). In his keynote talk, Boxer emphasized the need for the field to stay open to alternate hypotheses about how tauopathy progresses in different diseases, and how best to stop it.
“I continue to view tau immunotherapy as an important therapeutic strategy that should be further pursued, and I think we are still on the steep end of the learning curve,” Rabinovici wrote in a comment to Alzforum. “As we learned from anti-Aβ monoclonals, treatment approaches require a lot of fine-tuning before we see consistent results within a class.” In that vein, the field’s optimism has swung toward second-generation tau antibodies that take aim at tau’s midsection—particularly the microtubule binding repeats that drive aggregation (Mar 2021 conference news).
At CTAD, Biogen’s Hua Carroll talked about the first human study of one such newbie, BIIB076. Carroll did not say exactly where BIIB076’s target epitope is on tau, but did say the antibody is specific for extracellular forms that contain tau's mid-region. Carroll showed data of a single ascending dose study that tracked BIIB076's safety and pharmacokinetics in healthy controls and in people with AD. Five doses went into 24 healthy controls, and one into six people with AD who had evidence of amyloid. Twelve controls and two people with AD got placebo.
As doses were ramped up, safety concerns cropped up at the fourth-highest dose. Rather than proceed to a higher dose for the fifth group of controls, the researchers treated them with a dose midway between the third and fourth doses, and chose this for the AD cohort as well. A majority of adverse events—headaches, dizziness, nausea, vomiting, decreased blood pressure—were mild to moderate, but were more frequent in the higher-dose groups. One control fainted after infusion with the highest dose, accounting for the lone serious adverse event. Carroll called the safety profile of BIIB076 acceptable, and consistent with an older population.
BIIB076 engaged its target, halving the concentration of unbound mid-region-bearing tau in the cerebrospinal fluid of people with AD within one week of infusion. Three weeks later, the reduction persisted.
Can the tau immunotherapy field avoid the seemingly endless trail of failures that beset Aβ-targeted antibodies before things turned around? One way to speed things up is to go from sequential to parallel—i.e., platform trials. Oncologists use them, so does DIAN-TU, and at CTAD, Boxer unveiled his own plan. With Keith Johnson at Massachusetts General Hospital in Boston, and others, Boxer designed the Alzheimer’s Clinical Trial Consortium (ACTC) Tau platform trial, aka, ATP. It aims to test two tau-targeted therapies alone or in combination with an amyloid-lowering drug in a 2 x 3 factorial design that will share a placebo group.
The ATP proposal is currently under review at the National Institutes on Aging. The drugs have not yet been picked.
Tau Platform Trial. The proposed platform trial will test two tau immunotherapies alone or in combination with an anti-Aβ immunotherapy, in 900 people with preclinical or prodromal AD. One group, or about 17 percent of the trial’s participants, will receive placebo. [Courtesy of Adam Boxer, University of California, San Francisco.]
Participants with preclinical or prodromal AD will be prescreened for elevated amyloid using a blood test that measures the ratio of Aβ42 to Aβ40 and have amyloid and tau pathology confirmed via PET scan (Nov 2021 conference news). The trial aims to enroll 900 participants. It will run for two years and use change in tau PET as a primary endpoint. In essence, it aims to prevent the so-called “ca-tau-strophe.” Coined by Johnson, the term refers to the mushrooming of tau pathology that happens around the time symptoms emerge.
Why include anti-Aβ arms in a tau trial? For one, FDA approval of aducanumab, and perhaps others before long, means participants with early AD may want to take an anti-amyloid antibody rather than commit years to a tau drug they do not know will help them. Including several anti-Aβ arms, but only one placebo arm, offers participants a greater chance of receiving one or two therapies. Second, including both Aβ- and tau-targeted drugs in the trial will test whether two drugs given concurrently is better than either drug alone. Finally, inclusion of anti-Aβ drugs can serve as a positive control for biomarkers, Boxer said, because all of the anti-Aβ front-runners have been shown to influence tau PET as well as plasma biomarkers.
Rabinovici agreed that tau biomarkers will play a key part in moving the field forward. “I am optimistic that we will make rapid progress in evaluating the utility of tau immunotherapy, especially with our growing and maturing armamentarium of tau biomarkers,” he said.—Jessica Shugart
Lecanemab Sweeps Up Toxic Aβ Protofibrils, Catches Eyes of Trialists
With all the attention on aducanumab and donanemab these days (see previous stories in this series), lecanemab has been flying under the radar. Yet this often overlooked anti-amyloid antibody from Eisai/Biogen potently clears amyloid while producing less brain edema than its competitors. At the Clinical Trials on Alzheimer’s Disease conference, held in Boston and online November 9-12, Lars Lannfelt of Uppsala University, Sweden, made a case for lecanemab, aka BAN2401, being the strongest binder of aggregated Aβ among the current crop of anti-Aβ42 antibodies. Lannfelt led the BioArctic Neuroscience team that developed this antibody. Other talks at CTAD touted the consistency of lecanemab Phase 2 data, and added more evidence that it curbs tau pathology.
Lecanemab may soon become widely available; Eisai/Biogen have begun submitting data to the Food and Drug Administration to support its accelerated approval (Oct 2021 news).In the meantime, studies are ongoing, with this passive immunotherapy now in a trio of trials. CTAD speakers gave updates on screening improvements in the Phase 3 Clarity trial and the AHEAD 3-45 prevention study, which enrolls cognitively healthy people with amyloid plaques. Lecanemab has also been selected for the DIAN-TU Tau Next Generation trial, which enrolls people with an autosomal-dominant AD mutation. Tau NexGen will be the first trial to test combined amyloid and tau immunotherapies.
Randall Bateman of Washington University in St. Louis, who leads DIAN-TU, told Alzforum that combination therapy has long been the goal of the program. He believes the FDA’s approval of aducanumab opened the door for combination trials by creating demand for anti-amyloid agents. “The aducanumab approval changed the field’s perception of what is possible,” Bateman told Alzforum. “I think monotherapy trials’ days are numbered.”
Distinct Selectivity. Binding assays of three antibodies against different forms of Aβ indicate that lecanemab binds most strongly (dark gray) to protofibrils, while aducanumab and gantenerumab favor fibrils. [Courtesy of Linda Söderberg, BioArctic.]
A Protofibril Hog
Lecanemab differs from other antibodies in late-stage trials in that it was generated against synthetic Aβ protofibrils (Apr 2011 news). Protofibrils are large, soluble, β-sheet aggregates between 75 and 500 kD in size that are a major source of amyloid toxicity (Sehlin et al., 2012). By contrast, aducanumab was derived from the natural antibodies of healthy aged donors and recognizes aggregated Aβ, while gantenerumab was raised against fibrils. To pin down how these antibodies differ, Lannfelt tested them against each other in binding assays of Aβ42 monomers, oligomers, small protofibrils, large protofibrils, and fibrils. He used three different techniques: inhibition ELISA, immunodepletion, and surface plasmon resonance, where Aβ bound to a chip captures antibodies from solution. Lannfelt did not test donanemab, which recognizes a unique pyroglutamated form of Aβ truncated at the N-terminus.
Aducanumab was the weakest Aβ binder of the three. It did not recognize monomers or oligomers, and bound protofibrils transiently, with a fast on and off rate. It clung most strongly to fibrils. Gantenerumab also preferred fibrils over other forms, but did have some weak binding to monomers and oligomers, and glommed onto protofibrils as well. Overall, for both aducanumab and gantenerumab, binding strength increased with the Aβ aggregate size, but gantenerumab was the stronger Aβ binder no matter the species.
Protofibril Penchant. Inhibition ELISA shows that lecanemab binds small and large protofibrils with 25-100 times more affinity than does aducanumab, and 10 times more than gantenerumab. [Courtesy of Lars Lannfelt.]
Lecanemab had a different profile. It did not bind monomers or small oligomers, but did recognize larger oligomers in the 6- to 12-mer range, and it bound fibrils as well. However, it bound with the highest affinity to the mid-sized species, the protofibrils (see image above for three-way comparison). In head-to-head comparisons, lecanemab bound small protofibrils of 75-300 kD 10 times as strongly as did gantenerumab, and 100 times more than aducanumab. For larger protofibrils of 300-500 kDa, lecanemab bound 25 times as strongly as aducanumab.
If lecanemab mostly targets protofibrils, how does it clear fibrillar plaque? Lannfelt believes the antibody shifts the equilibrium in the brain by depleting soluble species. This would cause more Aβ to solubilize off plaques, dissolving these deposits, he suggested. Because Aβ can equilibrate between forms, targeting one species often affects others. For example, a prior study found that aducanumab suppresses oligomer formation by coating fibrils and preventing secondary nucleation of those smaller species on their surface (Sep 2020 news).
The different binding properties of each antibody may influence their clinical effects, Lannfelt noted. For example, ARIA, a type of brain edema caused by immunotherapy, may arise through antibodies binding to fibrils deposited along blood vessel walls, causing inflammation and leakiness of these vessels, he suggested. If so, lecanemab’s lower affinity for fibrils may explain its lower rate of ARIA compared to other antibodies, with an incidence of about 10 percent rather than 35.
Phase 2 Data Revisited
Why has lecanemab not gotten more attention? Perhaps it has to do with lingering concerns over the Phase 2 trial data. That study used an adaptive Bayesian design, which allows researchers to adjust parameters on the fly to favor the most effective dose, speeding up the trial (Nov 2012 conference news). The trial first read out at 12 months, but at that time failed to meet its prespecified endpoint of dramatically slowed decline on the ADCOMS composite (Dec 2017 news). By 18 months, however, lecanemab had slowed cognitive and functional decline by 30 percent on the primary outcome measure, similar to the performance of aducanumab and donanemab (Jul 2018 news; Jul 2018 conference news; Nov 2018 conference news).
Less Amyloid, Less Decline? In the lecanemab Phase 2 trial, the more plaque removed, the less decline in the ADCOMS. Data shows adjusted mean differences from the placebo group. [Image Courtesy of Eisai.]
At CTAD, Donald Berry of the University of Texas MD Anderson Cancer Center in Houston put these findings into context. Berry’s consulting group designs Bayesian trials, including the lecanemab trial. He noted that the goal of the 12-month endpoint was to show “super-superiority” over placebo, defined as an 80 percent probability that lecanemab would slow decline by 25 percent or more. At 12 months, lecanemab fell short of this, with a 64 percent probability of being super-superior to placebo. However, at this early point in time lecanemab was 98 percent likely to be superior to placebo, indicating there was a genuine drug effect.
Berry next addressed the robustness of the findings, analyzing the three cognitive endpoints—ADCOMS, ADAS-Cog14, and CDR-SB—using six different statistical methods. No matter the method or the end point, the findings were consistent, he found. In every analysis, the two highest doses of lecanemab, 10 mg/kg monthly and 10 mg/kg biweekly, were superior to placebo in a dose-dependent fashion. The ADAS-Cog14 was the most sensitive measure, with p values obtained by the six methods typically significant at the 0.01 level; CDR-SB was the least sensitive, with three of the six methods significant at the 0.05 level, and the others missing the mark. Overall, the consistency of the findings suggests a robust effect, Berry argued. He noted that regulators accept Bayesian designs for registration trials, and they have been used successfully in other fields, such as for Eli Lilly’s diabetes drug Trulicity.
Plasma Phospho-Tau Strengthens the Case
Eisai’s Chad Swanson added data from the open-label extension of this Phase 2 trial. Participants had been off lecanemab for an average of two years when the OLE started. As previously reported, the cognitive benefit seen on the highest doses was maintained over the time gap, and the banished plaques largely stayed gone (Dec 2019 conference news; Aug 2021 conference news). At CTAD, Swanson reported a strong association between plaque clearance in the OLE and slower decline on ADCOMS, with an eye-popping correlation coefficient of 0.83 at the treatment-group level. This contrasts with aducanumab Phase 3 data, where critics have pointed out a weak relationship between plaque clearance and cognitive benefit.
Plasma p-Tau Falls. Changes in plasma p-tau181 in people taking lecanemab mirror those previously reported for plaque clearance. [images courtesy of Eisai.]
New at CTAD were plasma p-tau181 data from this OLE. The recent availability of sensitive plasma biomarker tests is enabling researchers to mine new data from past trials, for example the analysis of plasma p-tau181 from the aducanumab Phase 3 trials (Nov 2021 conference news). Plasma biomarkers are also improving screening, such as the use of plasma p-tau in the Phase 3 donanemab trial (Nov 2021 conference news). For this OLE, Swanson reported that changes in plasma p-tau181 tracked with changes in amyloid PET and plasma Aβ42/Aβ40 at the level of individual participants. In the Phase 3 study, researchers will test whether plasma p-tau also correlates with the slowing of cognitive decline, Swanson said.
The relationship between plasma p-tau and brain amyloid suggests that lowering plaques slows tau phosphorylation, Bateman noted. “That’s encouraging from a biological standpoint,” he said, but added that these plasma biomarkers need to be validated with clinical and cognitive measures.
Christopher van Dyck of Yale University in New Haven, Connecticut, agreed that plasma biomarkers need further validation before they can be used to predict clinical outcomes. Nonetheless he was impressed with the lecanemab data, noting that the cognitive benefit maintained off drug strongly suggests a disease-modifying effect. “There’s a lot to like in these data,” van Dyck said.
Streamlining Screening to Bring Down Cost Lecanemab’s star may be on the rise, with the antibody now in three large trials. Swanson updated the CTAD audience on the Phase 3 Clarity trial, which now has 1,795 participants. Enrollment is complete in all 14 countries, except China. Demographics are similar to the Phase 2 trial, except the participants are more diverse. Phase 2 was 90 percent Caucasian, whereas Clarity’s population is 17 percent Asian, 13 percent Hispanic, and 3 percent black (Nov 2020 conference news).
Eisai’s Michelle Gee covered new screening procedures in Clarity. Screen failures are particularly costly for Alzheimer’s trials now because of the expense of PET scans. This can be minimized by using a tiered system that eliminates many applicants before imaging, Gee said. For Clarity, researchers developed a five-step process. In the first visit, participants provide a medical history and demographic data, and take three cognitive tests. These are the MMSE and the Wechsler Memory Scale Logical Memory tests I and II. About 35 percent of people who did not qualify for Clarity were eliminated at this first step, most due to their performance on the LM-II, which assesses delayed recall.
Step 2 comprises a physical exam, including ECG and labs, while step 3 adds an MRI scan. Relatively fewer screen fails happened at these stages—16 and 12 percent of the total, respectively. Step 4 is more comprehensive: Participants took numerous cognitive and functional tests and repeated the physical exam, MMSE, and Wechsler tests to obtain baseline data. Nine percent of screen fails happened at this stage. Only at step 5 did participants undergo amyloid and tau PET and/or lumbar puncture. Despite the extensive prescreening, 29 percent of screen fails happened here, mostly due to negative amyloid tests. Overall, 5,972 people needed to be screened to obtain 1,795 participants, a 70 percent overall fail rate. Still, Gee said the tiered system lowered cost and recruitment time as well as the burden on potential participants and study sites, since the majority of screen failures happened early in the process.
Likewise, Reisa Sperling of Brigham and Women’s Hospital, Boston, is refining screening methods for the AHEAD 3-45 secondary prevention trial of lecanemab. She found that prescreening using the plasma Aβ42/Aβ40 ratio helped select for amyloid-positive participants and dramatically cut down the number of PET scans needed (Nov 2021 news).
First Amyloid-Tau Combination Trial
The third trial testing lecanemab has a different design. DIAN-TU researchers had already planned Tau NexGen to be a tau-based study testing Eisai’s anti-tau antibody E2814 as the first of three trial arms when aducanumab received FDA approval last summer (Mar 2021 news; Jun 2021 news). Researchers surveyed DIAN participants, who carry inherited AD mutations that accelerate plaque formation, to gauge their interest in taking an anti-amyloid therapy (Aug 2021 news). The results were unequivocal: patients and families demanded access to anti-amyloid treatment, Bateman told Alzforum.
Researchers saw advantages in concurrent therapy, too. “We think tau therapy is more likely to succeed if we first remove amyloid plaques, which are driving tauopathy,” Bateman explained. Targeting tau in the continued presence of amyloid could be an uphill battle, Bateman said.
Now, participants will take lecanemab as well as E2814, but on a schedule that depends on their disease stage. Presymptomatic participants, who have less plaque, will take only E2814 or placebo for one year, as originally planned, then add lecanemab. Symptomatic participants will take lecanemab alone for six months to clear plaque, then add E2814 or placebo. This design will allow researchers to compare the effect of E2814 or lecanemab alone to the effect of both together. The trial will run for two years, with the primary endpoint being change in tau PET, and a secondary endpoint of CSF p-tau217. If these biomarkers are positive, the trial will run for two more years to assess cognitive change.
What about the other two arms of the Tau NexGen trial? Researchers have not yet chosen the therapies, but have decided they will hit different mechanisms, such as an anti-aggregation or tau anti-sense agent (Aug 2021 news). Whatever the tau drug, participants in all arms will take lecanemab. Bateman noted that one reason for selecting this antibody over others was because Eisai agreed to make it available for all subsequent trial arms, even those that evaluate non-Eisai tau agents. This allows researchers to use a single pooled control group, increasing the trial’s power, since everyone will be on the same anti-amyloid therapy for comparison. “All four [anti-Aβ] antibodies that clearly demonstrated evidence of amyloid removal were on the table. All had pros and cons,” Bateman noted. “It was a tough decision.”—Madolyn Bowman Rogers
Brain Shuttle Could Halve Amount of Gantenerumab Needed
Of the four anti-amyloid antibodies that abolish plaque, gantenerumab is the only one not yet applying for accelerated approval. Because its Phase 2 trials used too low a dose to dislodge plaque, this program does not yet have placebo-controlled data showing a slowing of cognitive decline. Even so, its Phase 3 program is advanced, with its two GRADUATE trials expected to read out late next year. At the Clinical Trials on Alzheimer’s Disease conference, held in Boston and online November 9-12, Roche’s Chris Lane presented their baseline data. Meanwhile, other Roche talks touted the company’s “brain shuttle” program, which ferries large molecules such as antibodies across the blood-brain barrier. New data suggest this strategy could double the plaque clearance a given dose of antibody achieves.
After the negative result of the Phase 2 SCarlet RoAD and Marguerite RoAD trials, Roche scientists explored different doses in open-label extension trials (Dec 2014 news). They found that fivefold higher dosing robustly removed plaque, such that participants became amyloid-negative within two or three years (Dec 2017 conference news; Dec 2019 conference news). Armed with these data, they picked a 1,020 mg monthly subcutaneous dose for Phase 3.
At CTAD, Lane described the scheme. Unlike in the aducanumab Phase 3 trials, all participants are being titrated up to the maximum dosage on the same schedule, regardless of their APOE genotype. Titration takes nine months, with the first three doses at 120 mg, the next three at 255, and the final three at 510. Because gantenerumab is injected subcutaneously, participants have the option of administering it at home, thus easing their time commitment and the burden of participating in a long trial.
The two GRADUATE trials are identical, but mostly run in different countries. GRADUATE I consists of 985 participants from 15 countries; GRADUATE II, 981 participants from 19 countries. Only the U.S. and Spain host both studies. The trials will take 27 months, having been extended for three months due to pandemic-related disruptions. Participants’ average age is 72, and their mean MMSE 24. Fifty-five percent of them have mild cognitive impairment, the remainder mild AD dementia. The population is somewhat more diverse than those of past trials, about 17 percent Hispanic, 12 percent Asian, and 3 percent Native American. However, like many other trials, there are almost no black participants. In part, this may be because diversity was largely driven by the countries participating, Lane noted. The study includes several Asian and South American countries, but none in Africa.
Unlike past trials, GRADUATE I and II will include hefty imaging substudies, Lane reported. About three-quarters of participants were screened for amyloid positivity by PET, and all of them continue to undergo longitudinal scans. All participants were invited into the tau PET substudy, as well, although Lane did not say how many joined.
While a subcutaneous jab has the advantage of being simple, scientists at Roche and elsewhere have been developing an alternative option for years. In this approach, gantenerumab is conjugated to an antibody fragment that recognizes the transferrin receptor, a major entry point through the blood-brain barrier. This is currently given as an infusion, and Roche declined to speculate whether it might eventually be a jab under the skin, as well. At AAIC 2021, Roche’s Luka Kulic had presented single ascending dose (SAD) results from a first-in-human study of this hybrid molecule, RG6102 (Mar 2021 conference news).
At CTAD, Kulic laid out the ongoing multiple ascending dose (MAD) phase of the study. It comprises four dose cohorts, with eight people on drug and two on placebo in each. Doses are 0.2, 0.6, 1.8, and 3.6 mg/kg, infused every four weeks. Participants will receive seven doses over the 28 weeks of the study, and then be followed for another 28 weeks. Unlike the healthy volunteers in the SAD phase, all MAD participants have either prodromal, mild, or moderate AD.
Besides measuring pharmacokinetics, -dynamics, and whether the conjugate provokes host antibodies, researchers will explore brain imaging by way of structural MRI, functional MRI, ASL-MRI to measure cerebral perfusion, and DTI-MRI to check the integrity of axonal tracts. They will also measure plasma and cerebrospinal fluid biomarkers including Aβ42, total tau, p-tau, NfL, neurogranin, and sTREM2.
Better Uptake? Preliminary human data on gantenerumab’s brain shuttle version (solid lines) indicates that it is cleared from plasma (blue) faster than a typical IgG (dotted lines), but reaches a higher concentration in cerebrospinal fluid (green) and could clear plaque faster (orange). [Courtesy of Roche/Genentech.]
How much might the brain shuttle boost delivery? Roche’s João Abrantes addressed this question by analyzing data from the human SAD study. To his surprise, he found the drug disappeared from blood at a rate of 2.0 L/day, almost twice as fast as expected based on prior data from monkeys, and much faster than typical monoclonal antibodies, which tend to top out at 0.5 L/day. Why might this be? Perhaps because more drug is moving from blood to brain in people. In support of this, the CSF/plasma ratio of RG6102 was 2.5-fold higher in people than in monkeys. These data suggest RG6102 has a higher affinity for the human transferrin receptor, increasing brain uptake, Abrantes speculated.
Based on these data, he estimated that 28 weeks of 3.6 mg/kg RG6102 treatment could lower plaque load about one-quarter from baseline. Alternatively, if the greater CSF exposure does not reflect greater brain uptake, and uptake is instead similar to that in monkeys, then plaque load would drop only by 12 percent in the same time period. This would be similar to the 15 percent clearance achieved by 10 mg/kg aducanumab in that time frame, Abrantes said. Results from the MAD phase will show which of these scenarios is true, he noted. This study is still enrolling and expected to end in the second half of 2024.—Madolyn Bowman Rogers
Young ApoE4 Carriers Have Reversed AD Proteomic Signature
APOE4 is the strongest genetic risk factor for sporadic Alzheimer’s disease, but at what age does the risk start to play out? A new study hints that it might be as young as one's 30s. In the November 10 Science Advances, researchers led by Madhav Thambisetty, National Institute on Aging, Baltimore, reported that 24 proteins upregulated in the brains of young adult APOE4 carriers are part of an AD proteomic signature. Curiously, these 24 proteins were downregulated in AD, while one other protein that was downregulated in young APOE4 carrier brains was upregulated in AD. The authors don’t understand this dichotomy. Still, levels of some of these proteins tracked with plaques, tangles, or cognitive decline.
Some of these proteins also are targets of approved drugs that have drawn interest for repurposing in AD. Two, the kinases Yes1 and Fyn1, are blocked by the anti-cancer drug dasatinib, a senolytic that is already being tested in Alzheimer's. At the Clinical Trials on Alzheimer's Disease conference held online and in Boston, November 9-12, Miranda Orr of Wake Forest School of Medicine, Winston-Salem, North Carolina, outlined the design of a Phase 2 trial starting this month. Called, rather graphically, SToMP-AD, aka Senolytic Therapy to Modulate the Progression of Alzheimer's Disease, it will test a combination of dasatinib and the anti-inflammatory compound quercetin in people with early AD. An ongoing, open-label study in AD suggests the combo is safe, Orr said. The work comes amid twin efforts to revive drug repurposing research in AD and to develop senolytic therapies both old and new.
Proteomic Signature
Orr praised Thambisetty’s approach, which compared proteomic signatures from different regions of the AD brain with those from young APOE4 carriers. “The use of tissue from multiple ages is important to appropriately interpret results and guide the development and use of therapeutic interventions,” she wrote (full comment below).
First author Jackson Roberts collected middle frontal and inferior temporal gyrus tissue from 62 people who had had AD and from 41 healthy controls in the Baltimore Longitudinal Study of Aging (BLSA) or Chicago's Religious Orders Study (ROS). Their average age at death was 89. Quantifying 1,300 proteins within the samples, the scientists identified 120 as either up- or downregulated in AD relative to controls.
Next, the scientists analyzed brain tissue from the Young APOE Postmortem Study; average age at death, 39. YAPS collects tissue from people who died of trauma and had forensic autopsies at the Baltimore coroner’s office. Co-author Juan Troncoso and colleagues at Johns Hopkins obtained samples from 18 APOE4 carriers and 17 age-matched noncarriers for APOE genotyping and storage.
Among the 120 proteins that together constituted the BLSA/ROS AD signature, 25 were expressed differently between the young E4 carriers and the noncarriers (see image below). “It is striking to see protein differences in E4 carriers decades before symptom onset,” said Giacomo Koch, Fondazione Santa Lucia, Rome, who participated in a panel discussion on drug repurposing at CTAD. The scientists don’t know if these carriers would have developed AD had they lived.
What do these 25 proteins do? Gene set enrichment analysis indicated some shared roles, including tyrosine kinase signaling. “Some signaling pathways, including inflammation, cell cycle arrest, and the autophagic-lysosomal network, suggest a role for senescence in the E4 and AD changes,” Orr told Alzforum.
Compare and Contrast. In AD brain tissue, 120 proteins were differentially expressed (purple and blue circles). Twenty-five of those distinguished young APOE4 carriers from noncarriers (orange circle). For the most part, expression change in E4 carriers (orange bars) was opposite that in AD (purple, blue bars). [Courtesy of Roberts et al., Science Advances, 2021.]
In the AD cases, 21 of the 25 proteins tracked with amyloid plaque deposition; 15 tracked with tau tangles according to Braak stage. Three of the 25 associated with slower cognitive decline via MMSE, and another three with faster decline.
Oddly, levels of all but one of the 25 proteins were more highly expressed in the young E4 carriers, but downregulated in the AD cases. Thambisetty thinks the changes in the young carriers may be driving the pathogenesis but in later years, as protein upregulation cannot be sustained over time, expression wanes. “Our results provide a window into very early biological perturbations occurring during the long preclinical phase of AD that may present novel therapeutic targets for disease modification," the authors wrote.
Of the 25 proteins, six turned out to be targets of existing drugs. They are tyrosine kinases Fyn1 and Yes1; the secreted lectin Lgals8; protein phosphatase Dusp3; the cytokine transducer Stat3; and topoisomerase 1. The scientists chose to study the Fyn1/Yes1 inhibitor dasatinib, which is FDA-approved to treat chronic myeloid leukemia (Lindauer et al., 2010). When treated with dasatinib, SH-SY5Y neuroblastoma cultures overexpressing a human tau fragment with the V337M and R406W mutations made less phospho-tau 231 and total tau (see image below).
Tempering Tau? In cell lines overexpressing human tau with tauopathy mutations, dasatinib reduced total tau (left) and phospho-tau 231 (right). [Courtesy of Roberts et al., Science Advances, 2021.]
Koch questioned whether hand-picking targets based on drug availability will work. “It is a bit of a long shot,” he said. “Just because drugs are available, especially if they are cancer drugs, does not mean they will be useful in AD if they are too toxic to take long-term.”
Another question is whether the proteins downregulated in AD would benefit from further quashing, as happens in kinase inhibition with dasatinib. MitziGonzales, University of Texas Health Science Center, San Antonio, called Thambisetty's findings encouraging but agreed that the opposite direction of expression between young E4 carriers and old people with AD highlights the disease's complexity. “We should be careful about timing potential therapeutics, because a drug that works in the preclinical stage may not work for clinical disease,” she told Alzforum.
For their part, Thambisetty's team will study dasatinib in mouse models and analyze existing clinical data for correlation between dasatinib use and cognitive problems via the Drug Repurposing for Effective Alzheimer’s Medicines study (Desai et al., 2020).
On the other hand, a Phase 2 senolytic trial run by Gonzales and Orr is starting to test dasatinib together with the flavonoid quercetin directly in AD (Gonzales et al., 2021).
“Identifying dasatinib at the convergence of two independent drug screens, one focused on AD pathogenesis and the other on senescent cells, is an exciting finding that lends support to the overall strategy,” Orr wrote.
SToMP to the Clinic
The combination of dasatinib and quercetin triggers cell death in senescent cells, i.e., cells that have outlived their usefulness but resist apoptosis (Gonzales et al., 2021).
In mouse models of tauopathy or amyloidosis, the drug combo has been reported to clear senescent brain cells, reduce tangle or plaque load, decrease neuroinflammation, slow brain atrophy, and improve memory behaviors (Sep 2018 news; Apr 2019 news).
SToMPing Along. A trial will give short bursts of low-dose dasatinib and quercetin to people with MCI and early AD, then follow up nine months later. [Courtesy of Miranda Orr, Wake Forest School of Medicine.]
SToMP-AD will recruit 48 people over 65 with MCI or early AD who test positive for tau by PET or CSF. They will take the drugs or placebo for two days, wait two weeks, then repeat, for a total of six rounds (see image above). Senolytic drugs are given intermittently because cells take time to become senescent. The dose is almost 10 times less than what is given for cancer.
After three months of treatment, the researchers will assess participants’ cognition and measure senescence markers in their blood. Measurements will be repeated at three, six, and nine months post-treatment, with a tau PET scan at the final visit. The primary outcome is safety, with secondaries of change in CDR-SB and ADAS-Cog, tau PET, and senescence blood markers. Recruitment is starting this month.
This regimen of low-dose bursts could allow patients to skirt the known toxicity of the drug. “So far, this low-dose dasatinib plus quercetin has been safe in three pilot studies, including our open-label pilot in older adults with AD,” Orr said. This pilot also tests if dasatinib/quercetin enters the brain. Five older adults with early AD took both drugs in the same intermittent cycles for three months, then had levels of each drug, total tau, Aβ42, and senescence markers measured in CSF and blood. MRIs were done at baseline and three months; CDR and MoCA at baseline, three, and six months.
At CTAD, Orr said that the final six-month follow-ups are almost complete, and that the regimen was safe. Gonzales, who leads this trial, told Alzforum that no one discontinued treatment and there were no serious adverse events. All other data analysis is ongoing. Gonzales plans to present top-line results at ADPD in March.
A separate open-label pilot, of the same intermittent dosing of dasatinib/quercetin in 20 people with MCI or early AD, is slated to read out in June 2023. Called ALSENLITE, its only outcome is safety. “So far [dasatinib and quercetin] seem safe in SToMP-AD and in ongoing studies for other indications, but it is too early to be assured,” study PI James Kirkland of Mayo Clinic wrote to Alzforum
Beyond dasatinib, research on senolytic compounds is growing rapidly. Kirkland is a co-author on an upcoming study led by Yu Sun, Chinese Academy of Sciences, Shanghai, that identified the flavonoid procyanidin C1 from grape seed extract as senolytic (Xu et al., 2021). Much of the paper focuses on cancer, but it also reports that intermittent administration of PCC1 to old mice reduced their burden of senescent cells, strengthened their physical activity, and lengthened their lifespans.—Chelsea Weidman Burke
The Rain in Spain: Move Over Higgins, AI Spots Speech Patterns
Could how a person speaks imply early cognitive trouble? My Fair Lady’s Eliza Doolittle would bristle at the question, but artificial intelligence might say it can, at least in people with frontotemporal dementia and Alzheimer’s disease. At the Clinical Trials on Alzheimer's Disease conference held online and in Boston, November 9-12, researchers presented apps based on artificial intelligence that detect subtle speech differences in the cognitively impaired.
One, from the Canadian company Winterlight Labs, picked up deterioration in how people with FTD describe pictures. Another, from U.K.-based Novoic, predicted mild cognitive impairment due to AD based on how well a person recalled a story they had heard. Others scientists devised an automated phone survey that assesses memory and executive function based on speech patterns, and are testing it in early AD. To fuel this type of research, the Alzheimer’s Drug Discovery Foundation will create a database of speech files, cognitive scores, and fluid and imaging biomarker measurements from 3,000 participants in six Alzheimer’s disease research centers.
“Speech biomarkers is an exciting field—imagine understanding if a person is at higher risk of FTD or AD just from the way they talk,” Foteini Orfaniotou, F. Hoffmann-La Roche, Basel, Switzerland, told Alzforum. Hiroko Dodge of Oregon Health & Science University, Portland, who is analyzing language patterns on recorded video chats with people 75 and older, agreed. “Speech biomarkers are very promising,” she said. Eric Siemers of Siemers Integration LLC thinks that figuring out who is amyloid-positive without a PET scan is the real promise of digital biomarkers, be they speech or cognitive tests.
Let’s Talk
Some people with FTD develop aphasia. They struggle to recall words, often resort to basic vocabulary, and construct simple sentences devoid of non-essential words. They pause or stutter. Jessica Robin from Winterlight Labs in Toronto said clinicians notice subtle language problems early in disease but have no tools to investigate what this means. Her company’s speech-assessment app aims to fill that gap, supplying an objective measure to complement cognitive rating scales.
Robin and colleagues developed algorithms that scored more than 500 vocal features across five categories. Language variables include: acoustics, such as pitch, pitch variability, and speed; lexical features, such as the types of words used, how common or evocative the words are, and the proportion of nouns to verbs; and syntax, including type and complexity of sentence construction. Other categories deal with the content of speech, including higher-order features such as how well a person stays on theme rather than bounces around verbally or repeats themselves, and fluency.
Cook Up a Story. This speech-assessment app asks participants to describe a household scene, and quantifies various aspects of the recorded speech. [Courtesy of Jessica Robin, Winterlight Labs.]
The researchers combined these scores into a composite that included vocal acoustics, how talkative people were, how often they paused, how often they used nouns, their sentence complexity, and the amount of correctly described picture content.
At CTAD, Robin presented results from an observational study of 36 older people with FTD. About two-thirds had the behavioral subtype; in them, language problems develop late in the disease. With the help of a caregiver, participants accessed the Winterlight app on a tablet or smartphone, and the app asked them to describe pictures in detail. They did this once a month for three months, then again at six, nine, and 12 months (see image below). The volunteers could take as much time as they liked, and provide as much or as little information as they wanted. “The open-ended format provides a rich snapshot of how people speak naturally,” Robin said.
Faltering Speech. In people with FTD, a speech composite score fell during the course of a year. [Courtesy of Jessica Robin, Winterlight Labs.]
Over the year, participants’ explanations of the pictures they were shown became briefer. They also paused more in their descriptions. This, along with changes in the other variables that make up the composite, lowered their scores (see image at right). “We were pleasantly surprised to pick up a number of speech changes over time, even in people with the behavioral variant,” Robin told Alzforum. Composite scores for 41 age-matched healthy controls held steady over six months.
Robin said she will study this app in larger cohorts, and compare scores to the “CDR plus NACC-FTLD,” a validated and publicly available composite measure that combined the original cognitive and functional domains of the CDR with behavior and language domains tailored to track FTD symptoms (Mar 2021 conference news). Robin also plans to correlate the speech composite with fluid and imaging biomarker changes. The Winterlight app is already used as an exploratory endpoint in a few AD clinical trials.
Do You Sound Amyloid Positive?
Researchers at London-based Novoic are developing an AI-driven speech app to detect not only MCI, but also amyloid positivity. The company’s Emil Fristed presented results from a study dubbed Amyloid Prediction in Early Stage Alzheimer's Disease From Acoustic and Linguistic Patterns of Speech. AMYPRED-UK pits the Novoic app against in-clinic cognitive assessments and amyloid biomarker analyses to see if the digital task can peg who has memory troubles and who has plaques (Fristed et al., 2021). The team recruited 71 cognitively normal old people and 62 with MCI or mild AD. Half of the participants had had a positive amyloid PET scan or CSF analysis within the past five years, while the rest had been negative within the previous 2.5 years.
During a baseline telemedicine call, participants took the Preclinical Alzheimer’s Cognitive Composite 5 (PACC5) test and completed an automated story recall task (ASRT) created by Novoic. For the ASRT, they listened to a 100- to 200-word story, immediately retold it, and repeated this with two new stories. The app recorded and auto-transcribed the reiterations, then scored them based on how closely they matched the original (Skirrow et al., 2021). Average scores from the three recalls correlated with MCI diagnosis about as well as did the PACC5 scores.
What about amyloid status? In the entire sample and in MCI participants, both the app and the PACC5 poorly correlated with amyloid no better than did demographics such as age, sex, and years of education. However, in cognitively normal people, the algorithm better correlated with amyloid positivity than did the PACC5 or demographics, though the effect was modest (see image below).
App Beats Doc, PET?The Novoic app story recall task (blue) predicted MCI (top left) as well as baseline PACC5 score (pink), while demographics alone (gray) did no better than chance. App and PACC5 similarly predicted amyloid positivity in the entire sample (top right) or MCI participants (bottom left), but the app better predicted positivity in the cognitively normal (bottom right). [Courtesy of Fristed et al., medRxiv, 2021.]
Fristed said they will wrap up analysis of all U.K. data and data from AMYPRED-US, a sister study being conducted in Santa Ana, California, by the end of this year.
You Rang, AD?
How early in Alzheimer's disease does a person's speech start to suffer? Alexandra König, University Hospital Center in Nice, France, Nicklas Linz at the start-up ki:elements in Saarbruecken, Germany, and colleagues want to answer this question over the phone. At CTAD, Linz described the Population-based Screening Over Speech for Clinical Trials in AD study. PROSPECT-AD uses a speech-based machine learning model to tease out subtle vocal changes and will test how they correlate with cognition, biomarkers, genetics, and family history of AD. The goal is to eventually use the phone as a remote screening tool for AD trials.
The researchers plan to enroll 1,200 participants 50 years and older who have subjective cognitive impairment or MCI and known amyloid and/or tau status. They will come from four longitudinal observational cohorts: BioFinder in Sweden, INSIGHT-preAD in France, DESCRIBE in Germany, and the EPAD site in Scotland. Enrollment is slated to begin early next year.
Participants will undergo in-clinic cognitive testing at baseline and after one year. Every quarter for 18 months, volunteers will receive an automated phone call that will guide them through the Rey auditory-learning and semantic-fluency tasks to assess memory and executive function. Answers will be recorded, and software will analyze more than 200 variables toward a composite score. Linz anticipates interim analysis in fall 2022 and final analysis by fall 2023. He said the phone test is already being used to prescreen participants in a Phase 2 AD trial, though he did not say which one.
Why a phone test rather than an app on a mobile device? “To capture speech, a phone call makes sense,” König said. The phone also enables wider screening because older people are likelier to pick up an occasional phone call and chat for 10 minutes than download and use an app regularly.
Building That Comprehensive Dataset
All these new speech-marker strategies are currently hampered by a lack of data on which to test their wares. Scientists are trying to build AI-driven algorithms capable of analyzing and picking out patterns among thousands of variables, but existing cohort studies do not come close to satisfying AI’s insatiable appetite for data on well-characterized study participants.
To plug this hole, the Alzheimer’s Drug Discovery Foundation will collect voice files through their Diagnostics Accelerator’s (DxA) Speech and Language Consortium. This longitudinal, observational study will recruit participants from ADRCs at Boston University, Emory University in Atlanta, and the University of Pennsylvania in Philadelphia, and from the Barcelona Brain Health Initiative and Barcelonaβeta in Spain, and Lund University in Sweden. Scientists will annotate the speech files with clinical, demographic, and biomarker data from the volunteers, collected annually. “We will have one common database for use as a single reference point,” Lampros Kourtis of ADDF said.
On a tablet provided by the study, 3,000 older people ranging from cognitively normal to dementia—either due to AD, FTD, vascular dementia, or Parkinson’s disease—will complete Novoic’s ASRT, complete a picture-description task, and answer a list of open-ended questions every quarter for at least three years. Responses will be in English, Spanish, Catalan, and Swedish, hence software will eventually be able to detect speech variables that change with cognition and are common across languages and accents.
A pilot study at BU and Emory is set to start up this year still; all sites should be enrolling by next year, said WHO. The dataset will be available in three to five years. “This is exactly what we need. The field as a whole will benefit from having a large dataset,” Linz said.—Chelsea Weidman Burke
Bringing Alzheimer’s Detection into the Digital Age
With a hefty shove from COVID-19, dementia scientists have accelerated their efforts to swap in-person cognitive testing for online versions. At the Clinical Trials on Alzheimer's Disease conference held online and in Boston November 9-12, advances in two areas were on display: moving existing assessments online, and creating wholly new digital tests that operate as smartphone apps. Using frequent remote check-ins, the aim is to detect mild cognitive impairment and even preclinical cognitive changes, without people having to come to a clinic.
Researchers presented data on a range of digital tests. The electronic clinical dementia rating (CDR) is the first attempt to move this established workhorse for staging dementia online. Other tests were new. The German company neotiv claimed that its smartphone app measures episodic memory and identifies early cognitive decline nearly as well as an in-clinic assessment. Likewise, a test developed by the Canadian company Cogniciti correlated well with the Montreal Cognitive Assessment. Roche reported preliminary-use data on its smartphone app, which combines cognitive testing with lifestyle surveys and phone-use monitoring to paint a fuller picture of cognition. Two other tests, the Computerized Cognitive Composite (C3) and the Boston Remote Assessment for Neurocognitive Health (BRANCH), are being developed at Brigham and Women’s Hospital, Boston. C3 predicted cognitive decline over a year; preliminary data on BRANCH suggest that it tracks how well participants learned and remembered tasks. Both might be used in prescreening for clinical trials.
Going Digital Yan Li of Washington University, St. Louis, and colleagues are bringing the CDR online. During this evaluation, an experienced clinician asks participants and, separately, their primary-care partners, questions to evaluate three cognitive and three functional domains. This requires a clinic visit typically lasting over 90 minutes.
To create an electronic version, the scientists chose questions from the CDR that easily could be adapted for automatic scoring. They kept verbatim those that required yes/no responses, while converting open-ended questions to multiple-choice when possible. In all, the eCDR has 47 questions for participants and 66 for informants, which can be completed in half and one-third the time of the in-person versions, respectively (see image below). Li previously reported that such a shortened version of the CDR retained much of the traditional one's accuracy and reliability (Li et al., 2021).
Faster Online. The in-person CDR takes 30, 60, and 10 minutes on average for the participant (blue), partner (orange), and clinician (green) to complete; the electronic CDR takes a fraction of the time. [Courtesy of Yan Li, Washington University, St. Louis.]
Next, Li plans to compare the eCDR directly to the CDR by administering both to 700 study volunteers who either are cognitively normal or have MCI, and their partners at four U.S. clinics. So far, 204 pairs have joined this four-year study, in which they will take the CDR in the clinic annually and the eCDR on their computer at home every six months. Participants and partners are told to take their portions separately. Li acknowledged that there is no way to verify the participant gets no help.
At CTAD, Li showed preliminary results of eight people with MCI and 39 controls from the University of California, San Francisco, comparing 49 eCDR responses to the corresponding answers from the CDR. For 35 of them, the correlation was tight, 11 boasting complete concordance. For the other 14 responses, disagreements between the eCDR and CDR might be due at least partly to technicalities, Li said. All those disagreements involved written responses that require the participant to agree with his or her partner to be scored as correct. Other questions revealed the difficulty of capturing a clinician's discretion. For example, for the question “Where were you born?,” a clinician might mark a participant's mere misspelling of the right city as correct, whereas the eCDR would label the response as incorrect. Importantly, all but one of the 14 most discordant answers were related to memory, rendering the correlation between the digital and tangible tests of this important domain the weakest (see image below).
All told, the eCDR correlated with CDR scores with an area under the curve of 0.86—the AUC being a statistical measure of correlation, with 1.0 being a perfect match.
CDR vs eCDR. Agreement between domain scores on the CDR and eCDR. [Courtesy of Yan Li, Washington University, St. Louis.]
The performance of the eCDRs’ memory domain is a problem Li and colleagues hope to improve by testing different types of questions. Randall Bateman, also at Wash U, wondered if probing subjective memory in the eCDR could do the trick. “Capturing subjective impression of an individual’s change over time is such an important part of what makes the CDR strongly predictive,” he said. Thus far, Li has excluded questions prompting a subjective response because the automatic scoring algorithm cannot analyze open-ended responses, but she hopes artificial intelligence may change that. Natural-language processing algorithms may be able to identify key words or phrases in responses and assess their quality and accuracy.
Eric Siemers of Siemers Integration LLC likes the concept of an electronic CDR, because it might overcome the limitations of in-person sessions. "I think an eCDR could eliminate some of the subjectivity that the CDR has, which is why you need so much training to be able to give it effectively,” he told Alzforum.
What About New Tests? Emrah Düzel of the German Center for Neurodegenerative Diseases (DZNE), Magdeburg, and colleagues at neotiv, a company he co-founded, are developing a smartphone app that probes episodic memory. It uses three tasks (see image below). The Mnemonic Discrimination for Objects and Scenes (MDT-OS) asks participants to discern if and how two pictures of a three-dimensional room are different. In the Object-in-Room Recall (ORR), the test taker sees two objects in a three-dimensional room and must identify them and where they were immediately, and again 30 minutes later. Complex Scene Recognition (CSR) involves identifying pictures as indoor or outdoor scenes and recalling after an hour which ones had been shown already. Each test takes 15 minutes.
Memory Triad. The neotiv app measures episodic memory using three tests. [Courtesy of Berron et al., medRxiv, 2021.]
At last year’s CTAD, Düzel had reported that ORR scores correlated with in-clinic neuropsychological test scores in 58 participants in the DZNE Longitudinal Cognitive Impairment and Dementia Study, a.k.a. DELCODE. Spanning healthy to AD, these volunteers have undergone extensive in-clinic cognitive testing, which makes them ideal candidates to evaluate a smartphone test. David Berron of DZNE, a neotiv co-founder, had said that ORR scores tracked with tau as per CSF and PET (Nov 2020 conference news).
This year, Düzel presented data from 102 DELCODE participants, including 25 cognitively normal people, seven cognitively normal first-degree relatives of people with AD, 48 people with subjective cognitive decline (SCD), and 22 with MCI as deemed by the CERAD neuropsychological test batter (Berron et al., 2021). The researchers compared a composite of their three tests against the parts of the Preclinical Alzheimer’s Cognitive Composite 5 that test episodic memory. Baseline PACC5 scores classified 29 volunteers as cognitively impaired, 73 as normal.
Participants downloaded the app onto a smartphone or tablet, and were asked to take one of the tests every two weeks for a year. After three cycles, they would have taken all three, which would generate a composite score. The study is ongoing. At the time of analysis, 87 participants had at least two composite scores. These correlated with baseline PACC5 scores and distinguished PACC5-defined normal from cognitively impaired people with an AUC of 0.9, a sensitivity of 83 and specificity of 74 percent (see image below).
Track with PACC. The neotiv composite correlated with scores from people the PACC5 had deemed cognitively impaired (red) or unimpaired (green). Dashed line denotes the app’s chosen cut-off; negative values mean worse cognition. [Courtesy of Berron et al., medRxiv, 2021.]
The scientists are monitoring how annual cognitive decline measured by their app holds up to PACC5 measurements in DELCODE. “PACC5 is sensitive to longitudinal change, and our digital tests have strong retest reliability, which are key to detecting decline over time,” Berron told Alzforum.
The Toronto-based company Cogniciti also develops digital tests. In its own effort to match results to established clinical testing, Theone Paterson of the University of Victoria, Canada, reported that portions of Cogniciti's cognitive test correlated well with in-clinic Montreal Cognitive Assessment scores in 40 cognitively normal adults and 51 with amnestic MCI. The digital face-name association and spatial working memory tasks predicted aMCI as accurately as did the MoCA, with AUCs of 0.76 and 0.71, respectively, Paterson reported at CTAD.
And Now for Preclinical Alzheimer's
Being more convenient than in-clinic tests, digital tests can be done more often. Kate Papp, Roos Jutten, and colleagues at Brigham and Women's Hospital, Boston, want to know if monthly checks can suss out subtle cognitive decline that yearly tests would miss. Papp asked 114 cognitively healthy volunteers from the Harvard Aging Brain Study to take the tablet-based Computerized Cognitive Composite (C3), which is a composite of the Cogstate brief battery, face-name associations, and an object-recall task. HABS volunteers did this once a month for a year (Aug 2019 conference news). They had amyloid and tau PET scans and in-clinic PACC5 testing at baseline and a year later.
This study's news had to do with practice effects, a known and nettlesome phenomenon in cognitive testing. All participants improved over the first three months of testing as they became familiar with the tasks, but these practice effects were smaller in people with high amyloid and tau burdens and in those whose cognition slipped faster on the PACC5. In fact, less improvement over the first three months on the C3 predicted who would decline by more than a 0.10 standard deviation on the PACC5 with an AUC of 0.91 (see image below).
Can't Outpractice the C3. Changes in C3 score over the first three months (blue line) predicted rapid decline on PACC5 better than did baseline C3 scores (green) or PACC5 scores themselves (orange). [Courtesy of Roos Jutten, Brigham and Women’s.]
Not wanting to wait months for a cognitive gap to emerge, Papp and Daniel Soberanes of Brigham and Women’s turned to daily smartphone-based testing. For one week, 101 cognitively normal HABS participants 65 and older took the BRANCH test, which includes face-name association, grocery item and price recall, and digit-symbol pairing tasks (Papp et al., 2021). Here, too, all participants completed the tasks more accurately as the week went by. However, older people and those with worse baseline PACC5 scores learned less well than did younger people and those with better PACC5 scores. “Early analysis of biomarker data has also shown learning-curve differences based on amyloid status, which we are excited to explore further,” Soberanes wrote via email. The neuropsychologists believe these subtle practice effects over the short term could flag participants who have subtle cognitive decline for early prevention studies.
More Than Testing
Beyond dropping pen-and-paper for the screen, some scientists are creating new assessments that encompass broader measures, such as a person's sleep quality, social engagement, or mood. Foteini Orfaniotou of Roche, Basel, Switzerland, showed preliminary results of a proof-of-concept study. Roche's app combines cognitive and motor-function tests with lifestyle surveys completed on a smartphone the company gives to volunteers (see image below). Orfaniotou said the surveys add insight into why a participant's performance may fluctuate from day to day.
Loads of Data. A Roche app measures how lifestyle factors (green) affect cognitive and functional activities (orange). Passive monitoring lets scientists track a person's engagement with his or her smartphone and his or her physical activity patterns (blue). [Courtesy of Foteini Orfaniotou, Roche.]
Aiming to study 120 volunteers eventually, the researchers thus far have enrolled 10 cognitively normal people, 51 with SCD, and 26 with early AD from three clinics in the U.S. and two in Spain. A complete data readout is planned for the first half of 2022.
Participants are assigned seven daily tasks/surveys for a month. Most had no problem using the app; two, who had early AD, did not finish the study due to technical problems or anxiety. Regardless of cognitive status, all completed at least one activity on 96 percent of the days. DZNE's Berron was glad to see this adherence and thought it boded well for digital tests. “I’m optimistic that we can implement [these tests] long-term, and in bigger groups, especially if the assessments are less frequent,” he said.
Remote Digital Tech as a Therapeutic?
In the COVID era, younger and middle-aged adults quickly turned to technology to keep their social connections despite physical distance. Older people who have been slower to adapt find themselves more socially isolated, upping their dementia risk (Aug 2017 conference news; May 2019 news). Could technology actually slow dementia, not just track it?
Hiroko Dodge at the Oregon Health & Science University, Portland, thinks so. Her prior pilot study found that 30-minute daily video chats for six weeks improved language-based executive function in cognitively normal 80-year-olds (Dodge et al., 2015). At CTAD, Dodge showed early results from the larger Internet-based Conversational Engagement Clinical Trial. In I-CONECT, 86 cognitively normal people 75 and older, and 100 age-matched people with MCI, signed up for four 30-minute structured video chats per week for six months, then two per week for another six months (Yu et al., 2021). Trained interviewers prompted conversation with pictures and asked participants to discuss related memories (see image below).
Chatting for Cognition. Through a simple interface on a provided laptop (left), older adults video-chatted with trained interviewers who prompted conversation with pictures (right). [Courtesy of Hiroko Dodge, Oregon Health & Science University.]
Among 31 people with MCI whose six-month assessment was available at the time of analysis, those who video-chatted maintained their baseline MoCA scores, while those who received weekly phone check-ins as a control declined. The researchers are now analyzing one-year follow-up data and other outcome measures, including changes in language-based executive function and speech characteristics. Among 25 cognitively normal volunteers, those who video-chatted improved in category fluency, a sign of better executive function.
Dodge thinks remote studies, such as I-CONECT, should combine digital cognitive tests with digital biomarkers, and analysis of speech patterns on the I-CONECT recorded video-chats is ongoing. “Identifying early decline in cognition by monitoring speech changes would be wonderful,” Dodge told Alzforum. (See Part 8 of this series).
Home or Clinic, or Home and Clinic?
Will any of this ever replace in-clinic tests? Alexandra Atkins, VeraSci, Durham, North Carolina, and colleagues think not. They asked 20 older adults with SCD and 41 age-matched normal controls to take the tablet-based Brief Assessment of Cognition (BAC), which includes symbol coding, verbal memory, visuospatial working memory, and verbal fluency tasks. The volunteers took the tests both in the clinic and at home. Some controls did unexpectedly better on verbal memory test at home, while all participants performed similarly on the other three tasks regardless of where they took them. Atkins did not speculate on why people did better at home.
This was but a small snapshot of the BAC, of course, which speaks to a limitation of digital cognitive assessments thus far—too little data, especially of the longitudinal sort. Rhoda Au, Boston University, noted that much of the current work is still trying to tease out patterns. “To get to digital biomarkers, we will have to invest as much effort as we have put into fluid markers,” she wrote to Alzforum.
Li noted that most studies these days are proof-of-concept to get a sense of what might be feasible and reliable. “Validation in a broader population is still needed to evaluate test performance,” she wrote. Sandra Weintraub, Northwestern University, Chicago, agreed. “Although a worthwhile effort, much work remains to be done to introduce these screens into practice,” she wrote.—Chelsea Weidman Burke
Papp KV, Samaroo A, Chou HC, Buckley R, Schneider OR, Hsieh S, Soberanes D, Quiroz Y, Properzi M, Schultz A, García-Magariño I, Marshall GA, Burke JG, Kumar R, Snyder N, Johnson K, Rentz DM, Sperling RA, Amariglio RE.
Unsupervised mobile cognitive testing for use in preclinical Alzheimer's disease.
Alzheimers Dement (Amst). 2021;13(1):e12243. Epub 2021 Sep 30
PubMed.

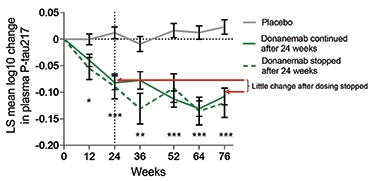


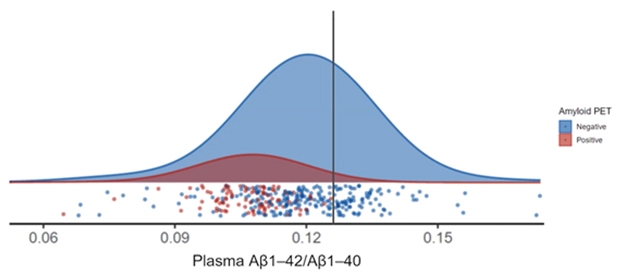

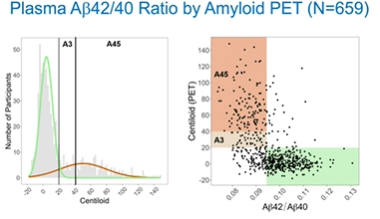


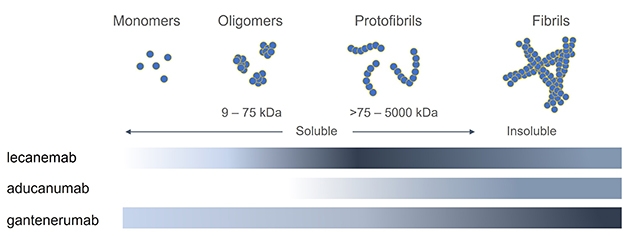

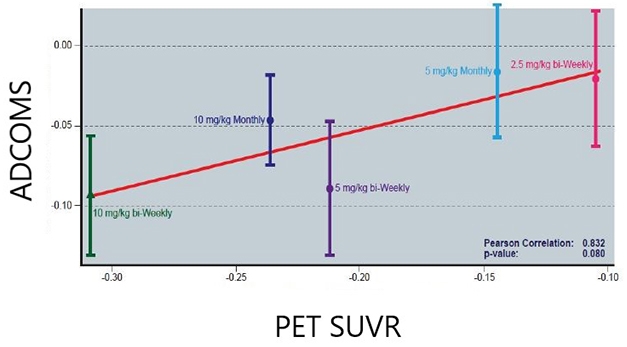
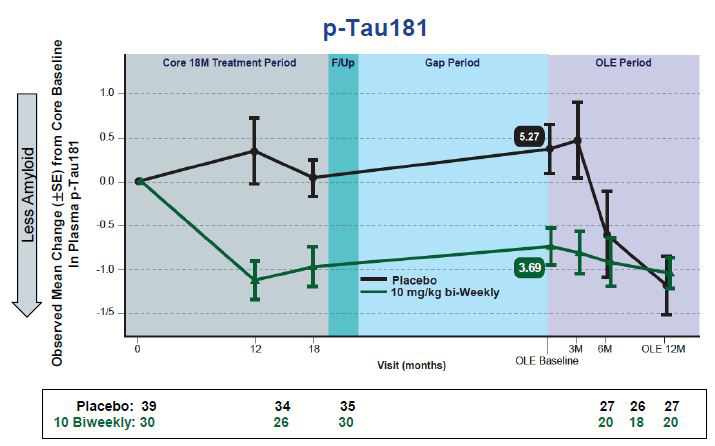

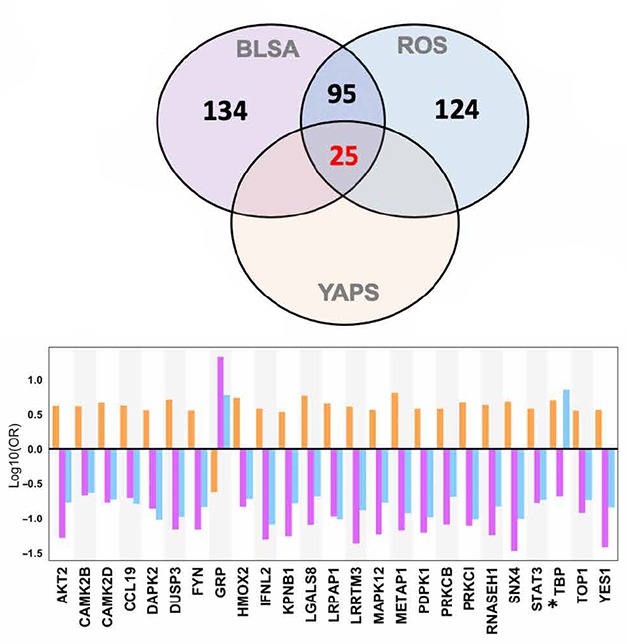
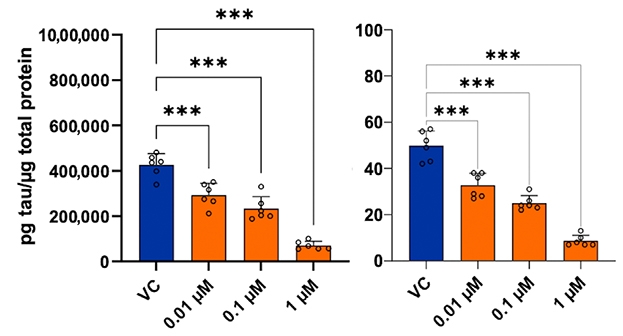
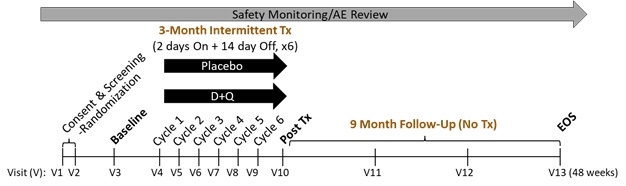









Comments
No Available Comments
Make a Comment
To make a comment you must login or register.