The ANN conference in San Diego covered such a plethora of topics, from anti-amyloid antibodies to IVIG, that organizers turned to breakout mini-sessions—what one scientist called "the neurological equivalent of speed dating"—to cram them all in.
Quick-and-Early IVIG Therapy: Hints of Promise?
If another small, hopeful trial is to be believed, pooled antibody treatment has the potential to stave off dementia. Eight weeks of treatment with intravenous immunoglobulin (IVIG), given to mildly symptomatic people deemed on the road to an Alzheimer’s diagnosis, just might slow the disease course. At least, the therapy slows shrinkage of the brain, according to preliminary results presented at the American Academy of Neurology meeting, held 16-23 March 2013 in San Diego, California. Following on other small Phase 2 studies that suggested a different intravenous immunoglobulin product could be beneficial for Alzheimer’s, Shawn Kile of the Sutter Neuroscience Institute in Sacramento, California, is trying this type of treatment in people with mild cognitive impairment (MCI). He hopes a short, early course of IVIG could delay Alzheimer’s dementia, although much further study will be necessary to confirm his hunch.
Doctors routinely use IVIG to treat a variety of infectious, immunological, and inflammatory conditions. The medicine is made from pooled plasma antibodies from donors, and among those antibodies are some that bind Aβ. People with Alzheimer’s possess unusually low levels of Aβ antibodies. IVIG is thought to work by promoting amyloid clearance and through its general anti-inflammatory effects. A previous Phase 2 study, led by Norman Relkin of Weill Cornell Medical College in New York City, suggested it could slow cognitive decline and brain atrophy (see ARF related news story), and several clinical trials are underway.
However, IVIG’s possible benefits come with a major potential caveat: The medication is expensive and in short supply, since it relies on donated plasma. If the treatment worked, Kile said, there would not be nearly enough of it to go around. In his study, therefore, he tried a shorter treatment course than others who have provided IVIG for 18 months or more to people who already have AD. Kile believed an early, brief therapy might suffice because in a previous study, scientists found that people who received IVIG treatment for reasons unrelated to AD were less likely to develop Alzheimer’s later (Fillit et al., 2009).
In Kile’s ongoing study, 52 people with MCI were evenly split between IVIG or saline placebo, receiving five doses spaced two weeks apart. Octapharma donated the IVIG but did not directly conduct the study. Kile used a dose of 0.4 gram IVIG per kilogram of body weight at each visit, based on the optimal dose from the earlier Phase 2 study led by Relkin. The total IVIG amount provided over the eight-week course matches standard dosage for IVIG treatment of neurological conditions such as the autoimmune condition Guillain-Barre syndrome, Kile said. He plans to follow the participants for two years. Thus far, 28 participants have hit the one-year mark, and Kile reported preliminary findings from that group in a poster at the meeting.
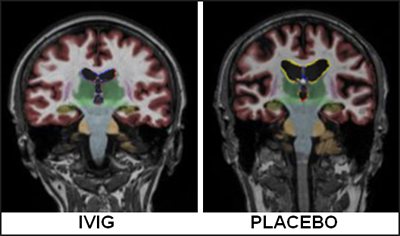
Comparing magnetic resonance images obtained at baseline and one year into the study, Kile observed that, while the placebo group lost an average of 8.8 percent volume, those on IVIG lost 5.7 percent, and the difference was statistically significant. “I was surprised; with a small ‘n’ we were able to show that,” Kile commented. Standard cognitive test scores changed little from baseline over the year. Based on the brain changes, Kile anticipates that cognitive decline may be noticeably slower in the treated group after more time has passed. This is at odds with immunotherapy results, where treated patients showed more atrophy than those on placebo, but it jibes with data from an MCI trial of B vitamins, which reported less atrophy in the treated group (Smith et al., 2010).
Magnetic resonance imaging showed that one year after treatment, people treated with IVIG (left) had less brain shrinkage than those on placebo (right). Image courtesy of Shawn Kile, Sutter Neuroscience Institute, Sacramento, California
The results confirm those of his earlier Phase 2 study, Relkin commented in an e-mail to Alzforum, although with a smaller effect on brain size. “If their final results prove to be consistent with these interim findings, it will likely spark a lively discussion about whether a short duration of IVIG is sufficient to obtain a meaningful therapeutic response in very mildly affected dementia patients,” he wrote. “A much larger study will be needed to draw firm conclusions about the use of IVIG in MCI.” (See full comment below.)
It is far too early to draw conclusions from Kile’s data, agreed Richard Dodel of Philipps University in Marburg, Germany, who has also worked with Octapharma’s IVIG (see ARF related news story on Dodel et al., 2013). He was skeptical that the final results would be positive. “This would be too good to be true,” Dodel put it. He also noted that change in brain volume is not a validated biomarker for AD, and it is not clear how that atrophy, or lack thereof, would affect thinking. “The cognitive measures are the most important measures at the moment,” Dodel said.
Kile’s group just completed dosing their last enrollee. As the study proceeds, he plans to analyze the rate at which people progress from MCI to full-blown AD.
Separately, researchers are also awaiting the results of a Phase 3 study of Baxter BioScience’s Gammagard® IVIG.—Amber Dance.
Anti-Amyloid Results Show Modest Benefits, Mild Side Effects
Scientists continue to squeeze every last bit of information out of Phase 3 trials for anti-amyloid antibodies solanezumab and bapineuzumab, even if the last droplets of news are small. Despite setbacks on the primary endpoint (see ARF related news story; ARF news story; ARF news story), researchers are still crunching numbers. They presented the latest analyses at the annual American Academy of Neurology (AAN) meeting, held 16-23 March 2013 in San Diego, California. Eli Lilly and Company's analysis of its two trials concluded that the solanezumab immunotherapy slows decline in cognition in people with mild Alzheimer’s disease, confirming an earlier independent analysis (see ARF related news story). And Reisa Sperling of Brigham and Women’s Hospital in Boston, with researchers from Janssen Alzheimer Immunotherapy of South San Francisco, California, reported a new, complete read of brain imaging data from the Phase 3 bapineuzumab trial. Looking for evidence of blood vessel damage they might have missed before, the researchers found several additional cases of amyloid-related imaging abnormalities (ARIAs). Those patients had not been taken off treatment. Overall, the ARIAs did not seem to herald worse outcomes, and are not necessarily a reason to stop anti-amyloid treatment, Sperling said.
Solanezumab Effects Confirmed
Lilly contracted the Alzheimer’s Disease Cooperative Study to analyze data from the EXPEDITION and EXPEDITION2 solanezumab clinical trials, which included 2,052 participants. The ADCS presented its results at meetings held in the fall of 2012. At AAN, Ann Hake of the company’s Indianapolis, Indiana, location offered the first public presentation of Lilly’s in-house analysis, which had been reported in a press release around the same time (see ARF related news story). The company’s strategy, designed prior to the trial, yielded results comparable to ADCS’, Hake said. “Apart from very slight differences … the results are remarkably similar.”
Based on pooled analysis of the trial data, the ADCS concluded last October that the drug slightly slowed decline in cognition and in performing daily activities in people with mild, but not moderate, AD (see ARF related news story). Lilly calculated that solanezumab treatment of people with mild AD slowed the rate of cognitive decline by 34 percent over the 80-week trial. Before the study, Hake noted, clinicians with whom Lilly consulted said a 35 percent impact on decline would be meaningful. “It is a modest effect,” Sperling commented to Alzforum, adding, “but if you do that five years before dementia, it could be extremely meaningful because you might be able to prevent dementia.” Lilly plans to initiate another Phase 3 trial, focusing only on people with mild AD (see ARF related news story).
Hake also presented a poster showing the effect of solanezumab on biomarkers. The ADCS previously reported that the treatment elevated total amyloid-β concentrations in plasma and cerebrospinal fluid (CSF), indicating the drug bound amyloid and removed it from the brain (see ARF related news story). Lilly's analysis agreed. The body takes a month to clear solanezumab-bound Aβ from circulation, Hake said, accounting for the many thousand-fold increase in total plasma amyloid in treated participants compared to those who received placebo. In the CSF, Lilly saw that solanezumab-bound Aβ went up while free amyloid went down, as expected. “The biomarker data showed evidence of target engagement,” Hake concluded.
Bapineuzumab’s Side Effects Extended
At the meeting, researchers reporting on Janssen and Pfizer's trial of bapineuzumab, focused on ARIAs. This worrisome side effect has surfaced in many immunotherapy trials. Poster presenter Nzeera Ketter from Janssen noted that when the intravenous bapineuzumab trial started in 2007, the researchers were not aware of the extent to which ARIAs would appear. Though ARIAs had occurred before in patients treated with AN1792, that trial was small, she said, and it used an active anti-Aβ vaccine (see ARF related news story on Hock et al., 2003). In addition, MRI scans were read by local radiologists at each trial site, and partway through the bapineuzumab study Janssen realized that those neuroradiologists had not identified every case of ARIA.
For the re-read reported in San Diego, neuroradiologists specifically trained to find ARIAs examined each of the 15,713 scans from the study of 2,400 people, looking for dense signals, or white spots on images, that indicate accumulation of extracellular fluid (see image below). They found 76 previously unidentified cases of ARIA, bringing the total for the study to 243. The missed cases were generally mild, Ketter said. Some people with ARIA had no symptoms associated with more severe ARIA, such as headache or confusion.
ARIA and Bapineuzumab
In some patients, treatment resulted in anomalous white areas on MRI images (bottom left and top right), indicating accumulation of fluid. However, as reported at the meeting, this side effect was not necessarily symptomatic. Image courtesy of Reisa Sperling, Brigham and Women’s Hospital, Boston
The researchers may have gained some serendipitous information from these 76 patients. Typically, when doctors noticed ARIAs in the trial, they put treatment on hold until they resolved, said Steven Salloway of Brown University in Providence, Rhode Island, who participated in the bapineuzumab program. But in these 76, treatment continued. Most ARIA signals went away by the next imaging session, about three months later and following another bapineuzumab infusion, but some returned, Sperling said. However, ARIAs affected neither cognitive nor functional tests, Sperling said in her talk. “ARIA is not as scary as we initially thought,” she told Alzforum, “but nevertheless, it does limit the dose we can administer, and we need to find a way to decrease the incidence if possible.”
Charles DeCarli of the University of California, Davis, asked if bapineuzumab may have worked in some patients but ARIA reversed its benefits. “Is that a group that might have done better, had they not had that effect?” he asked. Researchers agreed that it is difficult to know. While that is possible, Salloway noted that the data showed no treatment benefits that were reversed following the appearance of an ARIA.
More data are bound to come from both medications. A trial with subcutaneous bapineuzumab injections is still underway and, in addition to Lilly’s next Phase 3 trial of solanezumab planned for people with mild AD, the Dominantly Inherited Alzheimer Network is testing the antibody as a preventive treatment for mutation carriers (see ARF related news story), while the ADCS will test it in the Anti-amyloid Treatment in Asymptomatic Alzheimer’s Disease (A4) prevention trial (see ARF related news story).—Amber Dance.
Wrapping Up Enrollment, ADNI 2, PPMI Focus on Earlier Disease
On 18 March 2013 in San Diego, California—the site of this year’s American Academy of Neurology (AAN) annual meeting—the Alzheimer’s Disease Neuroimaging Initiative (ADNI) steering committee gathered to exchange the latest developments in this $140 million public-private project launched in 2004. About two and a half years into its second phase (see ARF related news story), the initiative is homing in on earlier stages of disease. The combined cohort from ADNI 1 and ADNI 2 will contain 350 people with mild to moderate AD, 550 with amnestic mild cognitive impairment (now called “late MCI”), 300 with early MCI, and 350 controls. Enrollment is nearing completion, said Michael.
Weiner of the University of California, San Francisco, ADNI’s principal investigator. Still needed are 40 more AD patients and 100 people for a new, even earlier cohort inspired by the Australian Imaging, Biomarkers & Lifestyle Flagship Study of Ageing (AIBL), called subjective memory concern (SMC).
In terms of baseline profiles, the newly enrolled early MCI cohort seems to fit “clinically right where we hoped,” said Laurel Beckett of the University of California, Davis, who leads ADNI’s biostatistics core. People with early MCI have Mini-Mental State Exam scores between 24-30 and a Clinical Dementia Rating (CDR) score of 0.5, with no dementia or significant functional impairment. On magnetic resonance (MR) measures of brain volume and positron emission tomography (PET) measures of glucose metabolism, early MCI subjects look more like the controls than the cohorts with late MCI, Beckett reported. On florbetapir PET measuring brain amyloid load, less than half of the early MCI group exceeds the cutoff for amyloid positivity.
With that, ADNI is shifting its attention toward even less impaired populations. “We are trying to move the clinical focus backward toward the very mild end of the spectrum. With an eye on a primary or secondary prevention trial, we want to stratify ‘normal’ people who may be on the road,” noted Ron Petersen of Mayo Clinic, Rochester, Minnesota, in an e-mail to Alzforum after the meeting. Petersen, together with Paul Aisen of the University of California, San Diego, heads ADNI’s clinical core. Thirty sites have received IRB approval to screen for this new SMC cohort, which got its first few subjects this past month. SMC is “meant to capture people who are ‘normal-ish,’” Petersen said. That is, they test as cognitively normal, scoring 0 on the CDR scale, yet have memory complaints registering as “mild concern” on the Cognitive Complaint Index used in Saykin et al., 2006 (see ARF related news story).
Leslie Shaw, who co-leads ADNI’s biomarker core with John Trojanowski, both of the University of Pennsylvania, Philadelphia, reported that the ADNI 2 CSF samples collected up until just days before the meeting should be uploaded onto the ADNI data site in mid/late April. This batch contains 680 samples—358 from ADNI 2, 242 from ADNI 1, and 80 from the GO carryover phase of ADNI 1. “Quality control continues to be a high-priority focus,” Shaw said. His team is working to harmonize methods and qualify mass spectrometry methods for characterizing Aβ peptides (see ARF related conference story).
As the number of manuscripts written using ADNI data soars above 600 and the number published pushes well past 350, it becomes critical to ensure that papers include sufficient detail for other researchers to reproduce results and compare them to other studies. Beckett presented to the steering committee a draft of reproducible research standards for ADNI publications. According to the new guidelines, authors need to provide a reproducible link for each source file they download from the ADNI data site. In addition, scientists must document all programming and statistical analyses with exact code or enough detail to replicate all steps of the analysis. “The pathway between program output and tables and figures in the paper needs to be transparent and reproducible,” the guidelines state. The plan is for these to be non-binding recommendations for some period of time, with a view to make them required in the long term, Weiner said.
Atsushi Iwata of the University of Tokyo gave an update on the Japanese ADNI (J-ADNI), a longitudinal biomarkers study that closely parallels the U.S. initiative. Launched in 2007, J-ADNI finished enrollment at 545 participants in March 2012, and 90 percent of the visits have occurred. The MCI-to-AD progression rate is 16 percent per year, a bit higher than in the North American ADNI. In addition, J-ADNI scientists report a slightly higher CSF Aβ42 cut point. Last fall, the second phase (J-ADNI 2) received approval for Japanese funding equivalent to $5 million over the next five years. J-ADNI 2 plans to start enrolling for 100 people each with early and late MCI this summer, Iwata reported.
In San Diego, Weiner also spoke about DOD ADNI, an analysis of brain aging in Vietnam War veterans funded by the U.S. Department of Defense. The study will use ADNI protocols to test if people with combat-related traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD) are at higher risk of AD than control subjects without these conditions. Research on the consequences of TBI and PTSD has intensified in recent years (see ARF related news series; ARF related conference story; ARF news story on Goldstein et al., 2012). DOD ADNI researchers will look for the following biomarkers as signs of elevated risk: higher brain amyloid load, lower cerebrospinal fluid (CSF) Aβ, higher CSF tau and phospho-tau, faster brain atrophy, and reduced cognitive function. The scientists hope to enroll 195 U.S. veterans—65 with TBI but no PTSD, 65 with PTSD but no TBI, and 65 controls with neither condition. People with mild cognitive impairment (MCI) or dementia cannot participate.
Given previous experience and expected dropouts, DOD ADNI plans to refer about 100 people for each of these groups to its 18 sites. Unlike in ADNI, individual DOD ADNI sites will not recruit subjects. Rather, the San Francisco VA Medical Center (SFVAMC) is handling this—a massive effort that has proven thus far more tedious than fruitful. Combing through VA compensation and pension records, SFVAMC last fall identified and mailed study brochures to thousands of veterans who met the broad criteria and live within 150 miles of a DOD ADNI clinic. The good news is that more than 350 subjects returned the reply card saying they would like to participate. The bad news: 168 declined once they heard more about the study in a follow-up phone call, and an additional 165 failed the initial screen. Excess metal in the body (e.g., from shrapnel, artificial joints, stents) makes MRI scans unsafe for them and accounted for a third of the screen fails. Another quarter came from people showing signs of both TBI and PTSD. DOD ADNI may end up enrolling some of these folks after all as part of a new cohort, given the slow recruitment thus far, Weiner said. At present, the study has enrolled 14 veterans; it needs about 180 more in the next 12-18 months.
To speed things along, DOD ADNI will hire additional recruitment staff and front-load critical information and questions to the early part of the phone screens. During the first few minutes, phone screeners will mention the lumbar puncture and other study details that tend to prompt declines, and ask about metal in the body. The advantage of the new approach is that a centralized phone bank performs much of the initial screening, which should reduce screen fails once the subjects arrive at the sites, Weiner said. Meanwhile, sites need to gain approval from the Alzheimer’s Disease Cooperative Study (ADCS). This process is also taking longer than expected because of additional steps and signatures required to certify the functional magnetic resonance imaging (fMRI) add-on to ADNI’s existing MRI protocol. Some sites will also collect diffusion tensor imaging (DTI) MRI data.
Ken Marek of the Institute of Neurodegenerative Disorders, New Haven, Connecticut, briefed the San Diego audience on the Parkinson’s Progression Markers Initiative (PPMI). This initiative launched in 2010 with goals and a design similar to ADNI’s (see ARF related news story), and some shared core personnel. PPMI now includes 24 clinical sites in the U.S., Europe, and Australia. Thirteen industry sponsors have committed approximately 30-40 percent of the $55 million needed for this initiative. The primary sponsor and funder is the Michael J. Fox Research Foundation for Parkinson’s Research. To date, PPMI has had more than 50,000 data downloads worldwide and 21 requests for biologic specimens.
“We are on the cusp of enrolling the full cohort,” Marek reported. At present, PPMI has more than 90 percent of its planned participants—400 people with newly diagnosed PD, 200 healthy controls, and 80 people in a newly added “SWEDD” (Scans Without Evidence of Dopaminergic Deficit) cohort. SWEDD subjects have PD-like symptoms but show normal dopaminergic brain scans, suggesting they are unlikely to have PD, Marek said. Reduced striatal binding of dopamine transporter (DAT) on SPECT imaging is required for entry into the PD group; however, about 15 percent of people screened for PD eligibility in PPMI have not met this requirement. In 2011, PPMI announced it would enroll these individuals and follow them for two years in order to compare their clinical and biomarker changes to PD patients with abnormal DAT imaging and healthy controls.
Unlike ADNI, PPMI participants must agree to lumbar punctures right from the get-go for CSF measurements at baseline and follow-up visits at six, 12, and 24 months. So far, this requirement has not hindered recruitment. Scientists have succeeded in getting CSF measurements in more than 97 percent of the participants at baseline, and 85-90 percent at six and 12 months, Marek reported.
PPMI has just started enrolling a prodromal cohort. In addition, it will begin recruiting LRRK2 mutation carriers this summer. Eventually, 500 LRRK2 subjects in PPMI will constitute the longitudinal study that was previously part of the LRRK2 Cohort Consortium (see ARF related news story), Marek told Alzforum. These 500 will be followed for three to five years, just like other PPMI subjects. The scientists plan to start collecting baseline data in July, Marek said.
Incidentally, ADNI’s data site has gotten a makeover, with a cleaner interface and new content, including data and samples overview tables (see MR Image Data page), ADNI 2 study updates, and more information on software and parameters, said Arthur Toga of UCLA, who heads ADNI’s informatics core.
The ADNI biostatistics core will hold the first session of a two-part online training on the use of ADNI data on Thursday, 4 April 2013, 8-10 a.m., PDT. The session will cover the basics of ADNI, including a brief overview of the study, navigation of study-related websites, data downloads, and use of visualization tools available on the LONI website. The training will emphasize where to find study details and how to make use of available resources. To register, please contact Naomi Saito.
In the ADNI spirit of collaboration and data sharing, slide presentations from the steering committee meeting are available on the ADNI site.—Esther Landhuis.
There were so many new data on neurodegenerative disease trials at the recent American Academy of Neurology meeting—held 16-23 March 2013 in San Diego, California—that organizers crammed some of them into an “Emerging Science Platform Session” of three-minute talks, chased with a brief poster session. “It feels like the neurological equivalent of speed-dating,” quipped C. Warren Olanow of Mount Sinai Hospital in New York.
65th American Academy of Neurology meeting. Image courtesy of Amber Dance
Speakers sprinted through talks on add-on drugs for Parkinson’s and Alzheimer’s treatments, as well as potential meds for amyotrophic lateral sclerosis (ALS). The biomarkers field was represented with a talk about cerebrospinal fluid (CSF) signals to nab subtypes of frontotemporal lobar degeneration (FTLD).
On your mark, get set, go!
Parkinson’s Relay
Four speakers showed drugs that could work on top of standard Parkinson’s therapy to boost quality of life. Jeffrey Cummings, of the Cleveland Clinic Lou Ruvo Center for Brain Health in Las Vegas, Nevada, led off. He ran a trial on a potential drug for the psychosis that complicates treatment of advanced Parkinson’s and forces patients into institutions. Pimavanserin is a 5HT2A receptor inverse agonist from Acadia Pharmaceuticals, Inc., of San Diego. The drug appeared effective in previous Phase 3 trials, but a strong placebo effect in those studies clouded the results. In the latest study, 199 people received pimavanserin or placebo for six weeks. Cummings said that this time, the drug met the desired endpoint, elevating scores on a PD-focused version of the Scale for the Assessment of Positive Symptoms. This scale is typically used in studies of schizophrenia. People who received the medicine had fewer delusions and hallucinations. They slept better at night and felt more alert during the day. These effects lightened the burden on their caregivers. Importantly, pimavanserin did not interfere with motor function, and was well tolerated. “Something like that is very much needed in Parkinson’s disease,” commented Juha Rouru of Orion Pharma in Turku, Finland.
Taking the baton, Olanow spoke about an add-on to levodopa treatment in hopes of shortening the time people with PD spend “off,” or frozen, when levodopa’s effects wear off. The Phase 2 trial tested tozadenant, an antagonist of the adenosine 2-α receptor, in 420 people who suffered an average of six “off” hours daily. Adenosine receptors modulate the release of neurotransmitters dopamine and glutamate. Two similar antagonists are under development, but tozadenant is less likely than those to increase blood pressure, said coauthor Uwe Meya, of Biotie Therapies Inc., in an interview with Alzforum. Meya works in the company’s Basel, Switzerland, office. The researchers tested four different doses and placebo. Taken twice daily, 120 and 180 milligrams were safe, cut “off” time by an hour, and improved Unified Parkinson’s Disease Rating Scale (UPDRS) scores. The researchers will consider these two doses for future trials.
For the next leg, Robert Hauser of the University of South Florida in Tampa presented a Phase 4 post-marketing trial of rasagiline for people whose symptoms aren’t kept in check with a single dopamine agonist. Over time, dopamine agonists may stop working, requiring higher doses that cause side effects such as sleepiness and poor impulse control. Rasagiline might help because it inhibits the enzyme monoamine oxidase B, blocking the breakdown of dopamine in the brain. Rasagiline is approved for early and late Parkinson’s disease, but few data exist in the literature to support doctors in prescribing it in mid-stage PD. Hauser believes people with PD “miss the boat” if they do not start taking it early on, he told Alzforum. Called ANDANTE, the study was funded by rasagiline's maker, Teva Pharmaceutical Industries Limited of Petach Tikva, Israel. Of 328 trial participants getting unsatisfactory results from dopamine agonist treatment, half received rasagiline, half placebo. Those on drug clocked an improvement in the UPDRS, particularly in motor function, Hauser said.
Stuart Isaacson of the Parkinson’s Disease and Movement Disorders Center in Boca Raton, Florida, took the final lap. He presented trial results for a drug to help the nearly 20 percent of people with PD whose blood pressure drops dangerously when they stand up (Ha et al., 2001). This effect is due to dwindling norepinephrine (Freeman et al., 2008), a hormone that signals the heart and blood vessels to control blood pressure. Chelsea Therapeutics, of Charlotte, North Carolina, makes a drug called droxidopa (aka L-DOPS; see ARF related news story) that is converted to norepinephrine in the body. In the 174-person Phase 3 study, people on droxidopa had higher standing blood pressure and felt less dizzy than those on placebo. This effect was statistically significant after one week of treatment, but not later on. “You may need to adjust the dose,” said Hauser, who was principal investigator on the trial. In the study, the dose was set after a two-week adjustment period. People on droxidopa were less likely to fall than people in the placebo group, and Isaacson was pleased to see that the treatment typically did not raise blood pressure to a dangerous level while patients were lying down.
Chelsea submitted a new drug application to the Food and Drug Administration in 2011, but the agency requested additional data and a demonstration that the treatment worked over a period of a few months. Initially, the FDA questioned whether the current study could satisfy their concerns. However, after an appeal from Chelsea, the agency recently said that the trial data presented might be sufficient for approval, with a possible requirement that Chelsea verify the durability of the benefits after marketing the drug (see the Chelsea press release).
Dementia Dash
On the dementia track, the drug ORM-12741 acts in a new pathway for Alzheimer’s drugs, blocking the α-2C adrenoceptor. Little is known about this receptor; in general, it “fine-tunes brain function,” said Rouru, who presented these results. Affecting many systems, the receptor is thought to modulate brain activity during stress. In rodent studies, ORM-12741 improved memory. In several Phase 1 human studies, the drug was well tolerated. At AAN, Rouru reported results from a Phase 2a study of 100 people with moderate Alzheimer’s. Those who took the drug for three months saw their scores on memory tests pick up by 4 percent, while people on placebo saw them drop by 33 percent in that time. The Orion group is planning another trial but has not set a date, Rouru told Alzforum.
Pivoting to frontotemporal dementia, speaker William Hu of Emory University in Atlanta, Georgia, addressed a conundrum in classifying FTLD subtypes. The disorder comes in two main varieties: lesions full of tau, or lesions made of TDP-43. “Currently, there is no reliable way to distinguish between these two while the patient is still living,” Hu said. “We really need to know what the underlying pathology is.” This would help researchers design clinical trials for drugs that target the appropriate pathology. The research team started with a set of 30 FTLD patients of known subtype at Emory. These were divided into tau and TDP groups based on autopsy, mutations associated with one subtype or the other, or secondary disorders typically linked with a subtype. MAPT mutations or progressive supranuclear palsy indicated the tau subtype, while progranulin or C9ORF72 mutations, or ALS symptoms, pointed to TDP-43. In this Emory cohort, the researchers discovered that the CSF ratio of phosphorylated tau to total tau was lower in the TDP-43 cases. They confirmed this pattern in a further 50 people seen by physicians at both Emory and the University of Pennsylvania in Philadelphia. Using the CSF tau ratio alone, they could identify FTLD-TDP with a sensitivity of 88 percent and a specificity of 73 percent. “We believe this will be very useful in designing future clinical trials,” Hu concluded. Researchers evaluating anti-amyloid drugs in AD have similar concerns about classifying participants properly; the emerging modus operandi is to ascertain amyloid pathology by CSF or PET before including someone in a study.
Not all racers were winners—one drug tripped up. Adam Boxer of the University of California, San Francisco, presented disappointing news on davunetide treatment for progressive supranuclear palsy (PSP). This neurodegenerative tauopathy affects people’s gait and balance, and causes a mild, progressive dementia. The drug, from Allon Therapeutics Incorporated of Vancouver, Canada, is a small peptide that was reported to be neuroprotective or to act on tau protein. Preclinical studies in tau transgenic mice were positive, as was a previous study in mild cognitive impairment, where the drug appeared to help working memory (see ARF related news story). Unfortunately, among the 313 participants in this international Phase 2/3 trial for PSP, davunetide was no better than placebo. At least, Boxer said, the work showed it is possible to perform trials in this rare disease. He reported that the dropout rate was lower than he had expected, and people generally complied with the study requirements. This was the pivotal trial for davunetide; Allon has said it is making no further plans with the drug (see ARF related news story; see also 27 March 2013 Allon update).
ALS Sprint
In the neuromuscular disease arena, Donald Sanders of Duke University in Durham, North Carolina, presented a Phase 2 trial of tirasemtiv, a muscle activator from Cytokinetics Inc. of South San Francisco. This study tested the treatment in 32 people with myasthenia gravis. The autoimmune condition interferes with nerve signals and weakens skeletal muscles, making it a good place in which to test tirasemtiv, said Cytokinetics’ Fady Malik in an interview with Alzforum. “We actually sensitize the muscle to neuromuscular input,” he explained (see ARF related news story on Russell et al., 2012). Single treatments with tirasemtiv improved muscle function in a dose-dependent manner. However, Cytokinetics is more interested in tirasemtiv to treat ALS, Malik said. Myasthenia gravis already has effective therapies, while ALS does not. The ongoing Benefit-ALS Phase 2 trial will examine tirasemtiv’s potential in 400 people with ALS.
Finally, researchers are also pursuing stem cell treatments for ALS. Dimitrios Karussis of the Hadassah Medical Center in Jerusalem, Israel, presented his work with Brainstorm Cell Therapeutics Limited of New York City and Petach Tikva. Brainstorm’s NurOwn therapy consists of bone marrow stem cells taken from each individual person, differentiated into cells that make neuroprotective growth factors, and infused back into muscle or the spinal cord. The researchers are halfway through a Phase 1/2 safety study intended to include 24 people. No worrisome side effects surfaced in six months of follow-up, Karussis reported. He was surprised, since it was a safety study, to also observe some hint of benefit. Participants’ rate of decline on the ALS-functional rating scale slowed after the implants, and muscle function and breathing improved. This mainly happened in people who received intrathecal implants. “I think it is promising,” commented Jinsy Andrews of Cytokinetics. She added that this kind of treatment could potentially help some people with other conditions, not just ALS, because the implants provide a general boost to neurons.
Brainstorm’s therapeutic differs from that of the better-known Neuralstem, Inc., of Rockville, Maryland, which is transfusing neural stem cells from fetal tissue into the spinal cords of people with ALS. Neuralstem has previously reported positive safety results (see ARF related news story and ARF news story).—Amber Dance.



Comments
No Available Comments
Make a Comment
To make a comment you must login or register.