CONFERENCE COVERAGE SERIES
International Conference on Alzheimer's Disease 2004
Philadelphia, Pennsylvania, U.S.A.
20 – 25 July 2004
CONFERENCE COVERAGE SERIES
Philadelphia, Pennsylvania, U.S.A.
20 – 25 July 2004
Brain imaging has emerged as perhaps the most promising source to date of an antecedent marker for Alzheimer's disease. Such a sought-after, tell-tale giveaway that the underlying process is marching along inexorably in people who do not yet have thinking problems could spot people who will most likely develop overt disease in the next few years. This could prompt them to adopt the modest preventive measures available to date, and perhaps expedite their access to clinical trials, as well as preventive and mechanism-based treatments as they—hopefully—come on line. A biomarker could sharpen the diagnosis of AD, and could monitor whether experimental therapies work. Finally, it could help test the major hypotheses of what causes AD more conclusively than is possible today.
Promising brain imaging approaches have sprouted up in many centers and labs. Attempts are underway across the field to achieve a consensus on which ones will prove to be the most useful in clinical trials and daily practice. The 9th International Conference on Alzheimer's and Related Diseases, held last week in Philadelphia, featured 306 presentations on various aspects of brain imaging. Rather than survey this still-scattered field, this conference story will summarize how a leading candidate is coming along.
Developed by Bill Klunk, Chet Mathis, and colleagues at the University of Pittsburgh, Pittsburgh Compound B (PIB) is a benzothiazole derivative that binds to β-amyloid in brain and is currently used as a PET imaging agent (see ARF related news story). Currently, six academic medical centers worldwide are examining the use of PIB imaging in AD diagnosis in small groups of patients and are conducting natural history studies of incipient AD. They are preparing to conduct larger studies. The Pittsburgh scientists are also planning to use PIB to monitor amyloid pathology in long-term HIV survivors who are developing AD-like pathology in what appears to represent a natural MCI model of sorts (see upcoming news story). However, PIB is not yet available to a wider public, and likely won’t be for at least another three years, Klunk emphasized at a press briefing at the conference. The compound has to clear technical hurdles and must be further validated before it can accompany large multicenter trials. For example, PIB imaging will not accompany the ongoing phase 3 trial of the anti-amyloid agent AlzhemedTM, said Paul Aisen of Georgetown University, who works on the trial.
What’s New with PIB?
In Philadelphia, the Pittsburgh team reported advances on several fronts in PIB development. For one, Mathis investigated a red flag that a separate group had raised when they found a metabolite of PIB in rat brain. This is worrisome because a metabolite lingering in brain could yield false-positive signals. Mathis analyzed blood and brain of mouse, rat, baboon, and human, and reported that, indeed, the troublesome metabolite did occur in rat brain but was absent from mouse or human brain.
For another, Klunk reported on another puzzle with PIB in animals. A problem hobbling microPET studies of PIB in transgenic mouse models commonly used in AD research—Tg2576, PDAPP, PS1/APP—is that PIB yields weak readouts even though these mice’s brains are loaded with Aβ. How could this be? Klunk and colleagues prepared brain homogenates of these models and tested PIB binding at the nanomolar levels used in imaging studies. The researchers found that about two moles of Aβ from human brain bind one mole of PIB, but that it takes 1,000 moles of human Aβ from mouse brain to bind one mole of PIB. “This may be important for nothing but PIB, or it might tell us something about the nature of Aβ aggregation in mouse brain,” said Klunk. Unlike in sporadic AD, mouse amyloid is driven by massive overproduction of Aβ. “In our hurry to aggregate Aβ in mice in a few months, something is not working in the same ways as in the real disease,” Klunk said. The difference could lie in Aβ modifications, chaperone functions, differences in kinetics. Whatever the explanation will prove to be, clearly β-sheet forms of mouse amyloid have a lower percentage of PIB binding sites than the real McCoy.
Pushing Back Diagnosis (Or “If it's a Duck…”)
In another presentation, Klunk showed data of an ongoing human PIB imaging study at the University of Pittsburgh. The researchers inject PIB peripherally and, minutes later, image brain amyloid in people with AD, MCI, and controls. Klunk reported on 15 initial cases. The five AD and control cases had values and imaging dynamics similar to the previous cases and controls reported in the older pilot study at Uppsala University in Sweden (see ARF related news story). More surprising were the data on the five MCI cases imaged to date. When lumped together into a group, these cases at first appeared to have PIB values intermediate between control and AD. But when plotted individually, the MCI cases separated completely, and each person fell either smack into the control group or the AD group. Data on such small numbers are clearly preliminary. Even so, they indicate that PIB can image MCI, said Klunk. Agneta Nordberg, of the Karolinska Institute in Stockholm, Sweden, presented similar results of MCI cases in the Swedish study.
Beyond that, this data separation speaks to an ongoing debate about what exactly is presymptomatic AD. The PIB result supports the view of John Morris, Washington University, St. Louis, that MCI is not a transitional stage between normal aging and AD, but that it already is AD, Klunk said. At the Challenging Views conference, held a day before the main conference, Morris and Jeffrey Cummings had debated Ron Peterson and David Bennett on the question of whether MCI is a prodromal condition from which some people progress to AD, or whether properly diagnosed MCI cases represent nothing other than early AD. Morris summed up his view by saying: “If it’s a duck, call it a duck!” Peterson holds that only a fraction of people with MCI will progress to AD, while others recover, stay stable, or come down with something else. He countered by issuing this advice to prevent an early AD diagnosis: “Don’t move to St. Louis!” While to the casual observer, the details of this ongoing debate have a slightly semantic whiff to it, the underlying issue of when to label incipient AD as indeed being AD has real consequences for clinical trial design and serious implications for the affected person (see also Morris interview).
What If? Would S(he) Have Gotten AD?
In theory, PIB imaging of MCI cases should be able to put to rest the circular argument that comes up when researchers discuss postmortem exams of people who died with florid amyloid pathology but no cognitive decline. Are these brains proof that amyloid is peripheral to the disease, a mere sideshow that has distracted research for too long? Or would these people surely have developed symptoms had they lived a few years longer? To address this question, Klunk and collaborators are planning to image normal elderly people to find those who have amyloid but no symptoms. “In natural history studies of cognitive performance with age, the older groups perform worse but their curve is quite broad. Many elderly actually perform very well. So the question we are now addressing with PIB is: Do the poor performers have amyloid? Once we identify them, we want to follow them to see if and when they progress to clinical diagnosis.”
In her talk about the ongoing Uppsala study of PIB, Nordberg presented first data on longitudinal PIB imaging, if not yet with presymptomatic people. A woman imaged two years ago at the age of 51, when she had mild-to-moderate AD, has in the meantime progressed to moderate AD clinically, and both FDG PET and PIB were able to track this progression. Maximum levels of PIB signal in human brain are not known, Klunk said.
Nordberg also presented new information on her study’s attempts to correlate PIB binding with CSF values of candidate biochemical biomarkers. The researchers found that PIB and CSF tau values correlated, but Aβ did not. This confirms a broader perception throughout the field that, to date, tau/phospho-tau appears to be a stronger candidate biomarker than Aβ.
PIB and the Vaccine Trial
These evolving data imply that amyloid-clearing treatments should start as early as possible, ideally before tau pathology as fueled by amyloid has taken a considerable toll on the brain, Klunk said. Can PIB improve the analysis of such treatments in trials? When an amyloid-removing drug fails, it is important to distinguish whether it had no clinical effect and no amyloid effect, or whether it had no clinical effect but a large amyloid effect. “These send you into different directions. In the first case, you’d want to make a better amyloid-removing drug; in the second, you’d conclude that amyloid removal does not improve the disease,” Klunk said. Toward this goal, Klunk reported initial data of using PIB on postmortem tissue of two cases in the aborted AN-1792 Aβ vaccine trial (see ARF related conference story). In one case, studied in Eliezer Masliah’s laboratory, amyloid had vanished from wide swaths of the frontal cortex. PIB binding in homogenates of these areas was down to control levels. The other case, by Isidro Ferrer (see Ferrer et al., 2004) was described as showing more spotty, focal amyloid removal, and PIB binding in homogenates of those areas fell just below that established for AD cases. "We are very encouraged that PIB binding will be able to detect immunotherapy-induced changes in brain amyloid," Klunk said. He added that the spotty amyloid reduction shows why scanning patients will be necessary to obtain precise results.
How early could PIB go? And exactly what forms of amyloid does it bind to in brain? “We don’t know,” Klunk said. “We have not yet found a good way to address what particular oligomeric forms PIB binds to. We know that PIB relies on β-sheet structure, so at some point an oligomer is going to be big enough to bind PIB, but we do not know at what point that is.” On the issue of which forms of amyloid species ought to be removed, Klunk cautioned against focusing narrowly on one species. A growing number of scientists believe that different Aβ species exist in an equilibrium, and that ridding the brain of one will affect the concentration of the others. For example, treatment of mice with antibodies against soluble Aβ tends to lead to a drop of insoluble Aβ, as well. “I see plaques as a landfill where Aβ has been thrown away. When you go in to clean things up, the remaining garbage pile begins to leach back out,” Klunk said. —Gabrielle Strobel.
One of the field’s biggest hopes for a quick and easy new AD therapy received a punch in the stomach today as the 9th International Conference on Alzheimer’s Disease and Related Disorders got under way in Philadelphia. John Breitner, of the Veterans Affairs Puget Sound Health Care System, Seattle, reported that three new prospective studies—together accounting for a mighty 30,000+ person-years of risk for AD—do not indicate any protection against future development of AD from prior statin use. This new work contradicts the original data linking statin use to reduced AD. What’s more, quite possibly this original data may have been an artifact generated because physicians prescribed statins less frequently to patients with dementia, Breitner charged provocatively. While ongoing treatment trials of statins in AD should continue, this new data weakens the argument in favor of launching costly prevention trials, Breitner argues.
Statins burst on the scene of AD research in the early and mid-1990s, when case-control trials reported that people who took these cholesterol-lowing drugs to prevent heart attacks and strokes appeared to have a lower risk of developing AD, too (e.g., Wolozin et al., 2000; Jick et al., 2000). By now there are seven such studies, and utterly unscientific surveys of researchers in the field (“Are you on it?”) suggest that many cognoscenti take these relatively safe drugs themselves with an eye toward preventing dementia down the line.
As is often the case when small epidemiological studies generate an intriguing new hypothesis, cell and molecular biologists began investigating mechanisms by which these drugs might act in AD. In the case of cholesterol and statins, scientists indeed have established solid in-vitro as well as mouse and guinea pig data showing, for example, that cholesterol and its related forms regulate APP processing. This would suggest that statins might be able to prevent AD, but data on the ability of statins to affect Aβ levels in humans are mixed. Basic science also has described cholesterol- and APP-independent effects statins may exert on processes relevant to AD, such as antiinflammatory or neuroprotective actions that result from the ability of statins to inhibit isoprenylation of a variety of proteins. The genetics front has done its small part by linking a half dozen genes related to cholesterol metabolism to AD, albeit in small studies that are not yet reproduced. Finally, hints of clinical success are on the horizon with small, published trials (Simons et al. 2002, Vega et al, 2004) and more recently a 12-month, controlled trial of atorvastatin conducted by Larry Sparks at the Sun Health Research Center in Arizona. This April, Sparks reported positive data at the Springfield Symposium in Montreal, where they were well received, but the full report of the trial is currently under review. Robustly stemming AD progression with a safe statin drug would be a sensational result, so researchers are eagerly awaiting publication of the full dataset of this trial.
While this good news is trickling in, however, epidemiologists trying to assess the potential of statins in AD more carefully have run into snags. To date, add-on studies looked for cognitive decline in three large, randomized, controlled trials of statins for prevention of cardiovascular disease. They are the Heart Protection Study of simvastatin, the PROSPER trial of pravastatin, and the CRISP trial of cerivastatin. All three failed to show any protection against dementia. Admittedly, Breitner said, the outcome measures used to indicate dementia were crude but even so, at least an inkling of protection clearly should have emerged from trials as large as these. In the Heart Protection Study alone, 20,000 people took drug, or placebo, for five years.
Here now is the disheartening news: Three new prospective, observational studies on AD also found no protective effect against AD. They are the ACT (adult changes in thought) study, the Cardiovascular Health Study, and the Cache County Study; two papers are in press, one is under review, Breitner said.
“The case-control studies were impressive, the prospective data are null. What is going on?” Breitner asked. He suggests the answer lies in the timing of drug exposure and measuring the outcome. The case-control studies were cross-sectional in nature, meaning they took data on exposed, unexposed, and demented cases in the same year. By contrast, the prospective studies asked specifically about antecedent exposure and AD ensuing later. Indeed, to simulate the early case-control studies, the authors took the original data from each of these three new studies and analyzed them as mock cross-sectional studies. Low and behold, now they saw a statistically significant (but entirely spurious) protective effect for statins from the same dataset that yielded a null result when analyzed properly.
The issue boils down to putting sufficient time between exposure to the test agent at hand, and the endpoint measured, i.e., incident AD, when trying to test prevention or risk reduction by that agent. Indeed, in separate addresses on other issues in AD epidemiology, Miia Kivipelto of the University of Kuopio, Finland, Lenore Launer of NIH in Bethesda, and Laura Fratiglioni of the Karolinska Institute in Stockholm, Maryland, all emphasized this same point. The case control studies compared exposed, unexposed, and demented cases in the same year, while in the prospective studies, cases are exposed to the agent under study, then there is a follow-up period of at least a year, and then scientists measure AD incidence. That is a key difference. “We need to time exposure to statins to the critical period of opportunity. We have not found that critical period and have no data in hand right now to do so,” Breitner said.
The major confounding problems in the original studies may have been prescribing bias by physicians, Breitner said. At the time the cross-sectional data was gathered in the early 90s, a doctor who saw a demented patient would have worried about the dementia more than about preventing a heart attack 10 years later. What’s more, at that time statins were new and not yet widely used. So Breitner and colleagues suspect that physicians simply prescribed statins less frequently to people with high cholesterol if they also had dementia. Yet this is not testable, Breitner noted, because today awareness and use of statins have expanded greatly.
In a related presentation, Murali Doraiswamy and colleagues at Duke University in Durham, North Carolina, described data from a small study examining what effect statin use had on hippocampal volume in elderly people with mild cognitive impairment. After two and four years of follow-up, neither hippocampal volume nor white matter was different in people who took statins from those who did not, indicating that statin use over this time period was unable to stem the hippocampal loss that is usually seen as people with MCI progress to AD.
The broader issues underlying this therapeutic approach saw spirited debate between Breitner and Ben Wolozin on the one hand, and Mary Sano, Larry Refolo, and Tobias Hartmann on the other, at the Challenging Views of Alzheimer’s Disease meeting held here in Philadelphia yesterday.—Gabrielle Strobel.
Perhaps…yes? At first blush, this is the tentative conclusion one must draw if the results of two presentations yesterday on the formal analysis of Elan’s AN-1792 vaccine are both right. The presentations were part of the 9th International Conference on Alzheimer’s Disease and Related Disorders, which ended earlier today here in Philadelphia. One group reported no overall cognitive improvement but upward trends in visual memory. Another jolted the audience by showing dramatic pictures of how patients who made antibodies in response to the vaccine clearly lost more brain volume than did patients who did not respond or were on placebo. Yes, you read it right: Responders had more brain shrinkage than non-responders. In the packed lecture hall, this counter-intuitive result led to a palpable sense of “I-told-you-so” and some snickering among those who doubt the wisdom of this approach. It left the presenters looking, for the moment, a bit sheepish as they tried to explain the paradox of how it could be that a treatment can stabilize thinking while apparently reducing gray matter. Last time most people checked, serial brain volumetry was considered a measure of continuing deterioration in AD.
The field has eagerly awaited results of this 27-center trial for two years, ever since dosing ended early because of encephalitis in about six percent of patients (see ARF related news story and ongoing Alzforum coverage since then). The surprising imaging result presented yesterday stirred up the audience enough to make this session arguably the liveliest in what has otherwise become a large and scripted conference that leaves little room for public discussion at the end of oral presentations.
Here is a summary of the data. Sid Gilman of the University of Michigan, Ann Arbor, first presented overall results of this phase2a trial of the AN-1792 vaccine containing pre-aggregated Aβ plus the adjuvant WS-21. The primary objective of the trial was to establish safety and tolerability, as well as first-pass efficacy data. “Responders” were pre-defined as patients who mounted an antibody response of a given size; the assessments included, among others, ADAS-cog, MMSE, clinical dementia rating (CDR), and brain volumetry. A secondary objective was to study the immune response generated by the vaccine, and changes in CSF Aβ and tau levels. The trial took place in the U.S. and Europe. Three hundred outpatients with mild-to-moderate AD who had had the disease for an average of four years received vaccine or placebo injections. The original protocol called for six shots, but after the encephalitis turned up, the company ended dosing so that the patients ended up receiving between one and three doses total (274 patients received two shots.) The investigators kept the study blinded for 12 months to exclude bias from the analysis.
Of the 300 patients, 59 mounted an antibody response. In the cognitive analysis, the investigators compared placebo, responders, and non-responders at baseline versus 12 months. Overall, they did not find significant differences between the placebo and responder groups, Gilman said. When investigators looked at performance in individual tests, they found that there appeared to be a trend. In four different Wechsler visual memory tests, those on placebo deteriorated as expected, while the responders showed small improvements, Gilman said. Only the result of one such test, the Wechsler verbal-delayed test, was statistically significant. In all other memory tests, the placebo group worsened more quickly than did responders, but none of these differences were statistically significant. Tests of executive function showed no differences.
When the investigators broke up the 59 responders into a group that made low antibody titers and one that made high titers, they saw no difference between patients on placebo and the non-responders, less decline in the low-responder group, and small improvement in the high-responder group. Subgroup analysis lowers power and tends to prompt heated discussion about what the numbers mean.
The CSF measurements showed no difference in Aβ levels but a reduction of tau in the responders. Most of the neuropathology findings were reported in this space already (see James Nicoll’s presentation in the ARF St. Moritz conference summary). The news since then is that two additional autopsy cases show broadly similar results. One, analyzed by Eliezer Masliah’s group at University of San Diego, California, showed focal depletion of plaques but persistent tangles, some lymphocyte infiltration and Aβ immunoreactivity. The other, presented here in Philadelphia in a separate talk by Nicoll, of University of Southampton in England, is of a person who died from a cardiac aneurysm only four months after getting the vaccine. That case shows considerable amyloid still in place but signs of active phagocytosis, i.e., abundant microglia surrounding the plaques with gobs of Aβ inside them, as well as some astroglia. In all, neuropathology on two cases with encephalitis and two without is available to date. The Masliah case is in press; for the second Nicoll case the manuscript is in preparation.
Overall, Gilman concluded that despite its difficulties, the trial had established a proof of concept that amyloid immunotherapy can elicit an immune response that leads to clearance of amyloid.
It was Nick Fox, of the Institute of Neurology, London, however, who delivered the big surprise when he presented results of the MRI component of the trial. The original protocol called for volume measurements at baseline, 12, and 15 months. After the encephalitis turned up, it was revised to drop the third scan. The investigators took three MRI measures. Whole brain measurement has relatively low resolution but the scan-rescan error is low and matching scan-rescan images has been automated. A patient with AD typically loses 20 to 25 milliliters per year, Fox said. Hippocampal measurement affords higher resolution but also has a higher error rate and requires manual outlining of the structure. AD patients typically lose three to six percent of hippocampal volume per year. Finally, ventricular enlargement complements the first two measures. It is less sensitive to artifact and changes by about 5 ml per year in AD patients, according to Fox.
The 288 patients who had paired scans included 57 on placebo and 45 responders. Fox said he reviewed all scans blinded to subject and time point. When the blind came off, the results fell out this way: Antibody responders had greater decrease in brain volume than did people on placebo. Correlation to titer showed that the more antibodies a patient had, the more volume they lost. Brain ventricles enlarged more in high responders than low responders. All three measures were highly statistically significant. High responders also showed more hippocampal loss, but this result was not statistically significant. Some people lost up to 60 ml from their brains. In relating brain volume changes to cognitive performance, Fox said that high responders had a better outcome even though they lost more brain volume and their ventricles enlarged more. They also had the largest drop in tau. The groups were balanced at baseline, and patients on placebo had volume changes exactly like what would be expected from the literature; non-responders fell in with those on placebo.
How to explain this surprising result? The brain volume loss could represent accelerated neuronal loss, perhaps as a result of sub-clinical encephalitis. Fox considers this unlikely because of the fall in CSF tau and the stable cognitive performance. Another possibility is that the brain collapses around areas of cleared amyloid, and the measured volume loss reflects the volume of the removed amyloid itself. Fox did not argue this point strongly, and questions from the audience and comments later on expressed doubt that the removed amyloid could account for this much volume change. There is disagreement about how much amyloid there is in brain, and ways of measuring it vary, but several researchers said that it is in the range of at most a gram. The brain loss could reflect fluids, or perhaps something else entirely is going on, some underlying qualitative change in the brain that the imaging did not visualize. See more on this puzzle below.
There has been intense research on various imaging approaches to diagnose and track the progression of AD. Indeed, brain volumetry has become a contender in the imaging field’s current efforts to agree on, standardize, and validate one or a couple of broadly accepted, robust measures as a consensus biomarker. To most casual observers, at least, shrinkage in cortex and hippocampus coupled with enlargement of the ventricles implies that AD is getting worse. But up until now, brain imaging research has been conducted separately from treatment trials, as trials are just starting to include a brain imaging component. Consequently, the apparent contradiction between cognition and imaging came as a surprise to many. Some researchers noted that perhaps animal studies of immunotherapy could help clarify this issue more quickly than future trials.
The session ended with this mischievous question from Peter Davies to Nick Fox: “If I treat a group of patients with an anti-tangle drug, will you cut me the same amount of slack?” Fox: “Yes!”
If you think the story ends here, hang on for three more paragraphs. Today, in the last session of the conference, Roger Nitsch of the University of Zurich presented the two-year follow-up in the analysis of the Swiss cohort of 30 patients, which his group conducts independently of the trial as a whole. This space has covered much of Nitsch’s presentation before (see ARF St. Moritz conference summary; ARF New Orleans summary). Here is what’s new since then: Nitsch’s team imaged their patients at the Zurich site, and they have completed a third scan on them. Like Fox, the Swiss researchers also see brain shrinkage, and the patients with the most robust cognitive stabilization had the most antibodies and also the most brain volume loss.
However, this volume loss ended after about a year, and the two-year scan showed a slight increase again. Then the team’s neuropsychologist conducted a Wechsler test of visual memory that draws on hippocampal function. “We have patients that are better now on it than they were at the beginning of the trial. I ask the audience, could this be a neuroregenerative effect?” Nitsch asked provocatively. It is important to note that at 2.8 percent (p=0.05), the reported uptick in brain volume appears to fall barely outside of the confidence interval. This group of high-responders numbers 11 patients, and all have had a second-year scan. It appeared to this writer as if the high responders and their comparison group who had not had an antibody response (n=3) did not start out with the same volume at baseline, so this data must be considered preliminary. Nitsch's group is continuing to follow their patients closely and expect to scan their brains again at future time points.
For now, Nitsch offered this speculative proposition: As the amyloid burden is cleared out, the brain also might shed some of the astrocytosis that typically accompanies AD. (In an earlier lecture at this conference, Stephen Paul of Eli Lilly and Co. had shown evidence suggesting that astrocytes clear amyloid; prior work on astrocytes and amyloid phagocytosis includes Wyss-Coray et al., 2003). The volume taken up by amyloid plus astrocytosis, plus other factors, would come closer to explaining the volume loss, Nitsch added. Privately, other neurologists agreed this possibility is worth testing.
Elan is continuing to develop immunotherapy approaches, as are academic laboratories and other companies. Elan has begun a phase 1 safety trial of a passive vaccine. As always, we invite comments and corrections.—Gabrielle Strobel.
APP and presenilin mutations cause Alzheimer’s, tau mutations cause tauopathies, and α-synuclein mutations cause Parkinson’s, right? Well, yes, but it’s not nearly that simple. At the 9th International Conference on Alzheimer’s Disease and Related Disorders, which ended yesterday in Philadelphia, Bart Dermaut at the University of Antwerp in Belgium presented an intriguing example of an exception to this neat separation. He described a man who had a presenilin mutation that gave him an otherwise classic case of a clinical/pathological tauopathy. This is not only mind-bending for those who still think in terms of these neat, simplistic categories. It is also but one of many examples illustrating the broader problem that, in real life, clinical symptoms, pathology, and genetics often just don’t match up, but create a bewildering spectrum of neurodegenerative diseases. Not least, such cases offer fascinating tie-ins to evolving mechanistic trends, such as the role of presenilin loss of function.
Dermaut works with Christine van Broeckhoven, whose lab tracks inherited dementias in adults and has uncovered great genetic and phenotypic heterogeneity among them, as have other groups. In Philadelphia, Dermaut related the story of a man who at age 50 lost initiative, became apathetic, emotionally blunt, and showed disinhibition of the frontal cortex (a polite scientific way of saying people behave embarrassingly and impulsively in public)—all tell-tale clinical signs of frontotemporal dementia (FTD). Brain imaging at that stage revealed atrophy in frontal and temporal regions of his cortex. At 59, the man’s cognition deteriorated severely; he died at 62. The gross pathology of his brain (dramatic atrophy, thinning of gyruses, ventricular enlargement) fit the pattern of FTD, and the molecular pathology (tau-positive Pick bodies and balloon cells in cortex) then led to a postmortem diagnosis of Pick’s disease as a subtype of the FTD complex. So far, clinic and pathology fit neatly into a little box.
But the genetics changed that. The man’s family history showed that his father had a slowly progressive cognitive deterioration, and a brother had had a personality disorder and taken his own life. Where one would have expected to find a tau mutation in this family, the researchers instead found a presenilin1 mutation. It segregated in the living family members in ways suggesting it is the right one. Of six younger siblings, some have the mutation but not (yet?) any symptoms. Though their clinical follow-up is still ongoing, Dermaut has noted mild atrophy in brain scans of some carriers, one of whom has clinical dementia. “We think this PS1 mutation causes this Pick version of tauopathy,” says Dermaut.
What is different about this PS1 mutation? Why did this man not develop AD? His pathology showed no amyloid plaques. The usual increase in the 42/40 ratio that most PS1 mutations cause appeared not to be there, either, though the presented data did not definitively answer this question. Closer inspection of this new Gly183Val mutation (Dermaut et al., 2004) yielded a clue, however. It alters a conserved base in the splicing signal at the sixth exon and leads to a splicing defect that leaves the PS1 protein without exons 6, or 6 and 7. This suggests that this heterogeneous form of neurodegeneration could be a splicing disease. Scientists Down Under have already found prior examples of this (see Evin et al., 2002). More broadly, several splice errors have been reported for some forms of AD, and they keep cropping up increasingly in other disease fields, as well.
“This short splice form of PS1 induces a non-amyloidogenic pathway that leads to a tauopathy,” said Dermaut. How would this happen? Dermaut had no answer but suggested that the mechanism may be related to presenilin loss of function. Samir Kumar-Singh, a member of van Broeckhoven's team, gave a separate talk about this unusual family, in which he pointed out that he found intracellular Aβ reactivity in autopsy brain tissue of a family member. Kumar-Singh analyzed the presence of tau in this brain and suggested that this PS1 mutation might interfere, directly or indirectly, with tau phophorylation or aggregation states. Furthermore, Dermaut pointed to a recent study, where deleting presenilin function in the cortex of mice led to tau hyperphosphorylation and neurodegeneration (see Saura et al., 2004 in ARF related news story). Beyond this published work, numerous disparate presentations in Philadelphia pointed to a loss of function for presenilin. As always, we invite our readers to fill the gaps in this story.—Gabrielle Strobel.
No Available Comments
If you’ve ever shone a flashlight through your hand and noticed what comes out on the other side, you have seen for yourself why red light could, in theory, make a medium for live diagnostics: It transmits better through thick, scattering human tissue than other parts of the visible spectrum. Brian Bacskai and colleagues at Massachusetts General Hospital in Charlestown, with collaborators at other institutions, have seized on this summer camp observation and are trying to develop an optical Alzheimer’s diagnostic. The researchers are not nearly there yet, but last week at the 9th International Conference on Alzheimer's and Related Diseases in Philadelphia, Bacskai briefed colleagues on how far they have gotten to date. “This would be a completely new approach,” Bacskai said.
Amyloid and tangle imaging agents including PIB (see ARF related Philadelphia story) and other compounds are under study at centers throughout the world. They hold great promise, but even if they progress through development and validation without major hiccups, they share the drawbacks of nuclear medicine. They require injection of radioactive compounds into a person’s blood and currently use positron emission tomography, or PET, which is expensive and not widely available. What if the same result could be achieved, more simply and cheaply, with optical techniques? One added advantage of optical imaging would be that an existing wealth of knowledge on the clever design of reagents might enable the synthesis of a highly sensitive probe, Bacskai added.
This project relies on near-infrared (NIR) laser scanning techniques to detect amyloid-binding reagents that fluoresce with wavelengths in the NIR spectrum. This differs from the multiphoton microscopy with which this research group has been imaging amyloid for a while (see ARF related news story). Multiphoton microscopy requires that the scientists make an opening in the mice’s skulls, and it can image tissue only in that small patch of brain up to about 500 microns deep. NIR imaging would be non-invasive and cover the whole brain, similar to PET or MRI. Indeed, NIR optical imaging is already being used in humans to detect breast cancer, visualize cerebral blood flow, and guide surgery.
(Click on the image to see the movie)This is a 3-dimensional volume of brain (615x615x 200micron) in an anesthetized Tg2576 mouse, recorded over time with multiphoton microscopy. A bolus injection of a novel long-wavelength amyloid binding contrast agent was administered via tail vein. The compound appears in the cerebral circulation, crosses the blood-brain barrier, and labels the cerebral amyloid angiopathy in this mouse brain within minutes. The goal is to develop even longer-wavelength fluorescent ligands for Abeta to allow non-invasive optical detection of amyloid plaques in vivo using near- infrared spectroscopy. (Image credit to Jesse Skoch and Brian Bacskai)
How far along is this project? The work focuses mostly on two parts: designing reagents and devising the detection schemes. The detection hardware is mostly in place, Bacskai said. Using commercially available instruments and NIR fluorescent reagents coupled to Aβ antibodies, the researchers performed proof-of-principle experiments in brain slices and whole brain. These showed that the scientists can detect a fluorescent signal deep in the brain and that it correlates with the mouse’s brain Aβ burden.
The next step is to synthesize a real-life diagnostic agent. It must cross the blood-brain barrier, target amyloid deposits specifically, and emit NIR light. This is what consumes most of the effort now, said Bacskai. Of the candidate compounds Bacskai described, some get into the brain and have high affinity for amyloid deposits, but their fluorescent wavelength is not far enough in the infrared (see movie above). Others are specific and fluoresce properly, but do not cross the BBB. None fill all three criteria yet. Stay tuned.—Gabrielle Strobel.
Updated 8 September 2005:
Last month, the researchers reported initial results from their collaboration with chemist Timothy Swager, Massachusetts Institute of Technology. According to the paper, the scientists developed a marker that binds to plaques and then fluoresces when exposed to radiation in the near-infrared range.
No Available Comments
Neurochem announced last week that it would halt development of tramiprosate (Alzhemed) in the wake of the failure of its large North American Phase 3 trial (see ARF news story and commentary). The Canadian company said it would immediately discontinue an ongoing European trial and put its resources into the development of a tramiprosate pro-drug that it claims achieves higher levels in the brain. The company will continue an open-label extension of the North American trial.
In a surprising twist to the story, the company said it plans to market tramiprosate, also known as 3-amino-1-propanesulfonic acid or homotaurine, as a nutritional supplement. CEO Francesco Bellini announced that Neurochem would form a separate company to sell this product. He said he expects this move to satisfy demand for the compound from patients and their caregivers, and to produce revenues to fund Neurochem’s continuing research and development activities.
The negative results of a multicenter North American trial came out earlier this year, and in August, Neurochem announced that the FDA would not accept alternative analyses of the data to compensate for problems with the trial. (Phase 2 and 3 trials between the FDA and sponsoring companies are confidential, and the FDA does not comment on them.) Barry Greenberg of Neurochem presented data from the North American trial last Friday, 9 November, at the Marian S. Ware Neurodegenerative Disease Research Retreat at the University of Pennsylvania in Philadelphia. The primary outcome measures of cognitive function showed no significant effect of treatment over placebo, but Greenberg reiterated that the ADAS-Cog and CDR-SB showed some numerical differences in favor of tramiprosate. He said that the company is getting hundreds of letters asking for the drug but cannot claim a treatment effect.
One measure did reach statistical significance in the post-hoc analysis, and that was hippocampal atrophy, Greenberg said. A subset of 312 patients out of the total 790 who completed the study had MRI assessments of hippocampal volume at the beginning and end of the study. Greenberg said that a preliminary analysis of the volume data by external statisticians found a dose-dependent reduction in hippocampal atrophy, after adjustment for confounding factors. Reportedly, a dose of 200 mg/day reduced atrophy by 65 percent, and the 300 mg/day dose halted atrophy over the 18 months.
“Neurochem is committed to analyzing and understanding the data generated in the North American trial,” Greenberg said. The company had initially hoped to use the lessons from the North American trial to improve the design of the European trial, but then decided to scrap it altogether. Instead, Neurochem will prioritize to accelerate development of NRM-8499, a pro-drug of tramiprosate. According to Bellini, that compound is in preclinical development, with results of toxicology tests in several animal species due in early 2008.
In his talk at Penn, Greenberg, as had Paul Aisen in his prior discussion of the trial’s woes (see ARF related news story), warned that problems encountered in the tramiprosate trial may stymie other researchers seeking to carry out large disease modification trials. Length, center variability, diagnostic uncertainly in mild AD, and lack of diagnostic biomarkers or surrogates for therapeutic effects all complicate the effort, Greenberg said. Added to that were limitations of psychometric measurements of cognition, most of which were validated for short-term effects. In addition, it is hard to quantify quality of life. “The clinical effect is ultimately the most important, but the tools we have are not matched to this. We need better tools with higher sensitivity,” Greenberg said. Borrowing a quote from Richard Mohs of Eli Lilly, a noted AD trials expert, Greenberg concluded by saying that trials evolve by dialog among all involved, and need to achieve both scientific rigor and clinical relevance. “It is time to reopen that dialog,” Greenberg concluded.
It should be added that, when put to leaders of AD programs in other pharmaceutical companies and academia, these scientists tended to reply that trials will succeed if the drug is effective. In addition, current trials of newer drugs are increasingly including biomarker measurements to gather the data needed for their validation. Off-the-record rumblings about a paucity of rigorous and relevant research data, either published or presented at conferences, had accompanied tramiprosate’s clinical development through the years.
Greenberg did not mention in his talk that Neurochem had announced the day before that they would pursue marketing tramiprosate as a nutritional supplement. When questioned about this, he declined comment, saying he was not involved in the decision or in any future work on those plans. In a webcast on 8 November, Bellini said the move was a reaction to the results of the trial, coupled to the “demands from physicians and family members for the drug.” Because it is a natural product, tramiprosate can be sold as a nutritional supplement without the need to establish safety or effectiveness, but it cannot carry therapeutic claims. Bellini claimed that tramiprosate could be on the market as early as 2008, but the planned subsidiary company has not been formed yet.
Could the marketing of a tramiprosate dietary supplement affect future trials of related compounds? This question will only be answered if the product hits the market and catches on with elderly people. Bellini placed the market for nutritional supplements geared toward cognition at a cool US$1 billion per year. No one knows what slice of this pie tramiprosate might eventually capture, and CEOs of struggling public companies have been known to make optimistic projections before. Neurochem’s share price tumbled from around $25 last December to about $2 following the FDA decision last August, and closed at $3.85 last Friday.—Pat McCaffrey and Gabrielle Strobel.
Of course mom was right; she always is. But for those who like evidence before they believe, consider this: At the Philadelphia conference, Francine Grodstein at Harvard Medical School presented data demonstrating that taking β-carotene starting in late mid-life protects later on against the kind of cognitive decline that heralds the beginning of dementia. This is the result of a cognitive function sub-study of the Physician’s Health Study, a large randomized prevention trial.
The rub lies in the length of exposure. The group who showed protection had been taking 50 mg every other day of β-carotene supplements for a whopping 18 years. A separate cohort who took it for approximately six years showed no benefit. This trial is one of the few to date that targeted the treatment at hand to a period in life when the underlying disease process had not yet begun or was truly at an early stage. (Researchers now believe this happens a decade or more before symptoms set in.) The trial also represents a vindication of sorts for antioxidant vitamins, which are generally thought to have some effect in staving off disease but have been disappointing in dementia-related trials.
The Physician’s Health Study (PHS) enrolls physicians, randomizes them to various treatments or placebo, and then follows them. The original PHS, of aspirin and β-carotene, began in 1982 with about 7,600 participants. It ended in 1998 and its result established low-dose aspirin as a preventive treatment against cardiovascular disease. At that time, β-carotene showed no protective effect, Grodstein said, and the trial continued. In 1997, the scientists recruited another cohort of physicians and randomized them to either β-carotene, vitamin E, vitamin C, or a multivitamin to ensure adequate folate levels. (Why physicians? To control cost, this trial relies on phone interviews to gather relevant information; physicians tend to provide that sort of information accurately and are considered highly motivated to participate long-term. Self-reporting is often cited as a technical weakness of other prospective studies, including the Cache County study.)
When the β-carotene arm ended in March 2003, the researchers assessed cognitive status in 6,012 people aged 67 and older: 4,118 from the original PHS and 1,894 new recruits. Ninety-two percent in each group participated in this assessment, Grodstein said; the others either refused or the scientists could not get them on the phone. The phone interview measuring cognitive ability comprised five tests including the East Boston memory test and a 10-word list. The primary outcome was a global composite score averaging performance across the cognitive tests. Risk of cognitive impairment was defined as being in the worst 10 percent of the performance distribution. This was pre-specified—something to keep in mind when reading epidemiological results. Frequently, when a study produces a disheartening null result in its pre-specified outcome, the researchers analyze it again for a second, more modest outcome, or they adjust their analysis to correct unexpected problems, such as a difference in the drug/placebo groups. Such results can be statistically weaker. Here, the two populations were identical in all measured confounding variables, as was participation in the cognitive sub-study.
The results showed that doctors who had taken β-carotene for about 18 years performed significantly better than did those on placebo (p= 0.2), and their risk of cognitive impairment was 20 percent lower (relative risk=0.81, 95 percent confidence interval). By contrast, the second cohort on short-term β-carotene performed just like those on placebo (p=0.5), and had the same risk (rr=1.09, 95 percent confidence interval). Performance differences were greatest in the verbal memory score, Grodstein said.
As far as epidemiological trial design goes, these data can be considered as showing strongly that long-term β-carotene helps maintain cognitive abilities and protects somewhat against dementia. The risk reduction was small, but given the prevalence of dementia in an aging population, delaying its onset by one year could eliminate several hundred thousand cases per year, Grodstein said.
The cognitive assessment measures researchers use in add-on studies to large trials fall far short of the clinical and neuropsychologic test batteries established for AD trials. Even so, Grodstein said, this phone interview is validated. “Poor performance on it correlates with later diagnosis of dementia,” Grodstein said. As a first-pass test of the interview’s relevance, the researchers determined the physicians’ ApoE phenotype, and it correlated with cognitive performance, Grodstein reported.
The length of exposure needed, and the long period of time between the exposure and the outcome in this study illustrate a problem that besets scientists investigating other experimental therapies, such as vitamin E, estrogen, or statins (see ARF related Philadelphia story). While the details of each case vary, generally good cell-, molecular-, and neurobiological data suggest these substances can help, but prospective observational epidemiology and treatment trials can come up empty-handed.
Consider vitamin E. Abundant biological data support the role of oxidative stress in neurodegenerative diseases, and at this meeting many more such data are pouring in. A prior two-year treatment trial reported an effect in patients with moderate AD upon adjusting the analysis (Sano et al., 1997), which prompted hope that perhaps this antioxidant would help earlier-stage patients even more. For this reason, vitamin E was included in the first treatment trial of MCI cases, led by Ron Petersen and Leon Thal. In Philadelphia, results of this trial (which will appear in this space in a separate story) were presented, and the vitamin E arm was negative. It did not slow the progression of people with MCI to full-blown AD at all. This looks at first blush like vitamin E does not work, and many people may spare themselves the expense now. The trouble is that vitamin E may still prove to be somewhat useful eventually, but this MCI trial exposed people to the vitamin only for three years, and perhaps too late in their lives.
Similarly, with estrogen the basic underlying science supports a protective role, but the Women’s Health Initiative Memory Study was stopped when both estrogen and estrogen/progesterone appeared to increase dementia (Espeland et al., 2004). One of the questions researchers are trying to sort out now is whether estrogen might help at earlier stages around peri-menopause, but hastens a disease process once it is underway. With statins, the current situation is puzzling in that prospective observational studies do not support the basic biology, either, though these studies may not have measured statin exposure nearly long enough (see ARF related Philadelphia story).
For β-carotene, surely cautionary remarks, qualifiers, and questions will surface. For example, might hearing loss have interfered with the assessment? Were the men in the first cohort younger than in the second when they started taking the vitamin? How could changes in dietary habits between the earlier and the later cohorts play into the result? This writer invites all readers to round off this conference summary with their comments and arguments.—Gabrielle Strobel.
No Available Further Reading
At the l7th Annual Marian S. Ware Neurodegenerative Diseases Research Retreat, held on 9 November 2007 at the University of Pennsylvania in Philadelphia, hosts Virginia Lee and John Trojanowski pulled together a formidable roster of speakers bearing news of big pharma’s efforts in the Alzheimer arena. In a rare summit of sorts, AD leaders from Merck, Pfizer, Wyeth, and Eli Lilly met to talk about the challenges and promises of developing new medicines to treat AD. About 200 researchers and clinicians from academia and industry showed up for updates on drug discovery for Alzheimer disease.
|
Barry Greenberg |
There was ample chance for discussion and commiserating about the difficulties of running AD trials, and the need for biomarkers, after Barry Greenberg of Neurochem presented data from the tramiprosate trial (see ARF related news story). Poignantly, Trojanowski asked how many failed trials before pharma loses its appetite for AD therapies? In answer, the presenters talked about strategies and targets too numerous to leave the observer with doubt about their commitment to the disease, where the need is so great and the market so large. If the day was any indication, they are all planning to keep on trying. |
|
Peter Reinhart |
What are they trying? Peter Reinhart, Senior Director of Neurodegeneration Research at Wyeth Research in Princeton, New Jersey, described his company’s strategy of moving forward on multiple targets simultaneously. The Wyeth pipeline includes both passive and active immunization approaches (see ARF related news story), inhibitors of Aβ production by both β- and γ-secretase, a plasminogen activator inhibitor (PAI)-targeted compound to boost Aβ degradation, and symptomatic treatments using neurotransmitter analogs. Reinhart said that Wyeth has a dozen candidate AD programs in the clinic, plus twice as many in preclinical stages. |
Reinhart highlighted two of these preclinical programs, a β-secretase inhibitor and a plasmin activator. In the β-secretase program, Wyeth identified selective, small, and potent inhibitors that knock down Aβ production in Tg2576 mice. Besides reducing plasma Aβ levels and brain plaques, the inhibitors produce a dose-dependent reversal of hippocampal-dependent memory deficits as measured by a contextual fear-conditioning trial. At the optimal dose of one such inhibitor, the AD animals remember just as well as non-transgenic animals, Reinhart said. The company is now trying to put their preclinical data together to move the inhibitor forward into human experiments. A recurring theme at the meeting was the uneasy dependence on mouse models for evaluating targets, with the outstanding question of how well those models predict important aspects of human disease. “Our initial clinical trials will only be as good as the models they’re based on,” was how Reinhart put it.
On the other side of the Aβ equation, Wyeth is also working on enhancing Aβ degradation by the protease plasmin, which chews up both monomeric and aggregated Aβ (see ARF related news story). Previous work has shown that Aβ aggregates induce tissue plasminogen activator (tPA), which cleaves plasminogen to yield active plasmin. There is evidence that the plasmin cascade is less active in AD. An inhibitor of tPA, plasmin activator inhibitor-1 (PAI-1), is upregulated in mouse models of AD and in human AD brain. Wyeth has identified small molecule inhibitors of PAI-1 that activate cleavage of Aβ in vitro assays. In Tg2576 mice, the inhibitor causes a dose-dependent decrease in plasma Aβ and reduces brain Aβ by about one-third after a single dose. Like the β-secretase inhibitor, the PAI-1 inhibitor reverses the memory deficits in the foot shock contextual fear-conditioning test. A naturally occurring mutation among some Amish families creates essentially a human knockout of PAI-1. These people have no obvious phenotype, suggesting that blocking PAI-1 may be a safe way to reduce Aβ, Reinhart said.
|
Seabrook, Lee, Hutton, Trojanowski |
Guy Seabrook, Senior Director and Head of AD Research at Merck’s site in West Point, Pennsylvania, talked about that company’s immunotherapy programs. This program includes an active vaccine based on a multiple antigenic peptide (MAP) vaccine |
construct. For passive immunotherapy, the company has recently focused on anti-oligomer antibodies, which they produced by immunizing mice with stable preparations of oligomers, or Aβ-derived diffusible ligands (ADDLs, licensed from Acumen). After affinity maturation and humanization, the scientists end up with highly selective anti-oligomer antibodies, Seabrook said. The antibodies preferentially block binding of ADDLs to cultured neurons, compared to Aβ monomers. When infused into rhesus monkeys, the antibodies elevated plasma Aβ. The speculation is that this Aβ is coming from the brain, which is consistent with data that the antibodies lower brain Aβ in several transgenic mouse lines, Seabrook said.
Merck is also actively seeking disease state biomarkers. On that goal, Seabrook showed results using CSF from subjects in the Oxford Project to Investigate Memory and Ageing (OPTIMA), in collaboration with A. David Smith of the University of Oxford in England. By combining information on the levels of Aβ42, tau, phospho-tau, and β-secretase, he said, his company achieved 99 percent accuracy in assigning AD in a group of elderly people with AD diagnoses confirmed postmortem.
In his keynote talk, Steven Paul, President of Lilly Research Labs in Indianapolis, focused on apolipoprotein E (ApoE) in AD. Despite being a well-established risk factor for AD, little is understood about how ApoE functions in the disease. AlzGene meta-analysis calculated that two E4 alleles elevate risk 15-fold, though a recent study with pathologically verified cases put that number as high as 25-fold (see ARF related news story). How does the E4 protein, which differs by just two amino acids from the protective E2 isoform, increase risk so dramatically? Paul thinks if researchers can sort out the role of ApoE4, the pathogenesis of AD will become much clearer. Earlier work by Paul, Kelly Bales, and Ron DeMattos at Lilly and their collaborator David Holtzman at Washington University in St. Louis, Missouri, has shown that human ApoE effectively reduces Aβ deposition/amyloid plaque formation in aging PDAPP mice. The ApoE2 and ApoE3 isoforms are more effective than the ApoE4 isoform. Consequently, Paul and colleagues have postulated that drugs that increase ApoE expression or secretion in the CNS may prevent or slow the progression of AD (see ARF related news story).
What is clear is that cholesterol transport pathways are intimately involved with the production and clearance of Aβ in the brain. ApoE is the major lipoprotein in the brain, where it is made mostly by astrocytes and microglia. With recent work showing that the lipid transporter ABCA1, which is required to transfer cholesterol to ApoE, also functions in Aβ clearance, both ABCA1 and ApoE have become important drug targets. Agonists of the liver X receptor (LXR), a steroid receptor that regulates the expression of both genes (Liang et al., 2004; Lefterov et al., 2007; ARF related news story), have been proposed as therapeutics. However, Paul cautioned, the approach may require selective compounds that would stimulate expression in brain more than in peripheral organs to avoid unwanted side effects such as a fatty liver.
ApoE may also play a role in the inflammatory response to Aβ, Paul showed. When the researchers exposed PDAPP brain slices to astrocytes in a culture dish, they found that astrocytes from adult mice avidly degraded Aβ. The adult cells picked up Aβ via receptor-mediated endocytosis in a process that requires ApoE; astrocytes from ApoE knockout mice did not do it, Paul reported.
In the wake of reports that peripheral monocytes can enter the brain and phagocytose Aβ (see ARF related news story, but see also ARF news story), Paul and his coworkers tested the effect of peripheral macrophages on the brain slices. They found that the peritoneal macrophages gobbled up Aβ without harming the brain tissue. These cells took up Aβ from diffuse plaques, but also ate amyloid, whereas neither microglia nor astrocytes could destroy amyloid. Similar to what the scientists saw with astrocytes, macrophages from ApoE knockout mice were far less effective in clearing Aβ or amyloid than cells from wild-type mice. And when macrophages expressing the human ApoE isoforms were tested, E2-expressing cells proved much better at clearing amyloid than E4-expressing cells. The activity of the Aβ-degrading enzyme matrix metalloprotease 9 was higher in ApoE2-expressing macrophages than in E4 expressers. “ApoE2-expressing macrophages are plaque-eating machines,” Paul said. Paul’s results jibe with recent reports from several groups about clearance of plaque by brain-infiltrating macrophages (see ARF related news story and ARF related conference story). Now, Paul’s group is trying to replicate the results in vivo by transplanting bone marrow from E2-expressing mice into PDAPP mice, to see if those cells can clean up plaque.
Michael Hutton of Merck presented an alternative to the Aβ-centric view in his talk on tau-targeted therapies. Hutton recently left academia to take a position as Senior Director of Neuroscience Drug Discovery at Merck Research Labs in Boston, where he is in charge of non-Aβ-directed therapies for AD.
Hutton said that arguments in favor of targeting tau in AD only start with the fact that tau pathology exists side-by-side with amyloid as a hallmark of AD. Tau itself can cause neurodegeneration, as evidenced by the 20 primary tauopathies caused by familial mutations in tau. In addition, tauopathy correlates with neuronal loss and memory decline, and its proximity to neurodegeneration may mean that tau therapies offer the best chance for disease modification. Mouse models with robust neurofibrillary tangle pathology show widespread neurodegeneration, cell loss, and functional decline, which might increase the likelihood that they will be good reporters for therapeutic effects compared to amyloid-only models. In addition, multiple rare tauopathies (considered orphan diseases) present the opportunity for proof-of-concept studies, and Hutton said he feels a responsibility for including these patients in clinical studies. Finally, elevation of phospho-tau, a validated biomarker in AD CSF, could provide a simple way to monitor therapies.
The downsides of targeting tau include its key role in microtubule function and its propensity to form intracellular lesions. In AD, no tau mutations are known, and only a weak association of risk is seen with the tau H1c haplotype variant, suggesting that tauopathy may play but a peripheral role in the disease. So far, findings in tauopathies do not show a clear pathogenic mechanism, and cell models for tauopathies are poor, Hutton said. Despite the availability of transgenic mouse models, no unambiguous or consistent therapeutic prevention or disease modification studies have been reported. Hutton said that may just be because the field is still young.
Even with these drawbacks, potential tau-directed therapies abound: kinase inhibitors, aggregation inhibitors, reducers of tau expression, and microtubule stabilizers are all possibilities that are under study in various labs. Enhanced clearance of tau by HSP90 inhibitors is another angle (see ARF related news story). Hutton noted his surprise that even tau immunotherapy shows some promise (see ARF related news story).
|
Christopher Austin |
Tau aggregation inhibitors have been identified in several high throughput screens. Hutton highlighted one from the Mandelkow lab in Hamburg (Pickhardt et al., 2007), and Christopher Austin, director of the NIH Chemical Genomics Center, talked about two more at his center. As part of the Molecular Libraries Screening Initiative, Austin’s lab screens a growing library of more than 200,000 compounds, and has developed “quantitative HTS.” This method allows the government scientists to |
use multiple concentrations already in a first screen of each compound, rather than one high concentration, as is done in many screens. By going right to dose-response curves, Austin says, his group saves time, identifies many more positive hits, and can come out of a first screen with structure-activity relationships. “This method has revolutionized our ability to draw conclusions relatively rapidly after screening,” Austin said. Last year, working with Jeffrey Kuret of Ohio State University in Columbus, they identified compounds that either inhibited or enhanced tau aggregation (Honson et al., 2007). Now, Austin says they are working with Virginia Lee on another large-scale screen of tau.
|
Holly Soares |
Nearly every speaker expressed a wish for better biomarkers, both to nail an early diagnosis and to quickly assess the effects of new treatments. As Trojanowski put it, “We are not going to get very far very fast without ways to monitor disease with biomarkers.” With that, he introduced Holly Soares, a Director of Translational Medicine at Pfizer Research in Groton, Connecticut, who talked about her group’s work on serum biomarkers. |
Interest is high in blood-derived markers, with their promise of easily accessible, non-invasive diagnosis or tracking of disease progression. For example, a panel of 18 proteins was recently described by Tony Wyss-Coray and coauthors (see ARF related news story) that could distinguish elderly people with AD from those without. Those markers were discovered by measuring a larger group of 120 proteins and then comparing disease and control samples to find the set that discriminated the two populations.
Soares described a similar approach, comparing blood from 20 patients with mild to moderate AD and 20 matched controls. Blood was tested at 3, 6, and 9 months, using HumanMAP from RBM in Austin, Texas, a bead-based multiplex assay for 89 different proteins that included cardiovascular risk factors, inflammatory, and cancer markers. Of the proteins assayed in the recent Wyss-Coray paper, 44 percent were also included in the Pfizer experiment. Their test found no discriminatory power for AD versus control in these overlapping analytes. Soares said they had trouble with variability in the inflammatory markers, but did see changes in lipoproteins and tumor necrosis factor α between cases and controls. She said the beads can differentiate AD versus control plasma, but not with the same set of proteins that Wyss-Coray and coworkers reported. Soares did not see changes in the profiles over time, at least up to 1 year, but wants to do longer studies.
In another study, Soares showed data on biomarker measurements in serum samples from Pfizer’s Alzheimer Disease Cholesterol-lowering Treatment trial. That trial tested the cholesterol-lowering drug atorvastatin, and in a small study the scientists looked at the effect of cholesterol-lowering on several potential biomarkers. They saw little or no changes in plasma Aβ levels or ratios. A brain-specific cholesterol marker, cerebrosterol, was decreased in patients on the drug. When Soares applied the multiplex assay, she found significant decreases in serum amyloid P, a potential seed for amyloid fibrils, in the patients on drug. That was unexpected, and may reflect different mechanisms of action of the statins, beyond their effects on cholesterol synthesis via HMG-CoA reductase. The multiplex assays are very powerful, Soares said, because they can give a fuller picture of the effects of drugs in the context of a disease. She concluded with this optimistic assessment: “Finding biomarkers in plasma is not easy, but they are there.”
At the end of the day, John Trojanowski observed that no one had addressed the issue of trying to slow aging. What did pharma think about setting aside specific AD targets and going after aging pathways, such as the resveratrol approach? This topic seemed to be on the speakers’ radars, but still just as a blip, caught at the early stage where people are thinking about how to design animal models to test anti-aging pathways.—Pat McCaffrey.
One of the basic research flavors that wafted pungently through the 9th International Conference on Alzheimer’s Disease and Related Disorders last week in Philadelphia is the growing sense that intraneuronal Aβ may have more of a hand in Alzheimer’s disease than previously appreciated. No one doubts that it must exist; after all, APP cleavage occurs in intracellular membrane compartments. But the discovery in the early 1990s that neurons secrete Aβ, as indeed do cells in most tissues of the body, drew much attention to its extraneuronal forms. What’s more, intraneuronal Aβ is rarely detected, whereas extraneuronal Aβ plaques are there in plain sight. (Similarly, the field’s overwhelming focus for many years on plaques rather than smaller species, such as oligomers, owes much to the fact that plaques are visible and thus amenable to study, while oligomers are maddeningly elusive in vivo.) This meeting report summarizes some of the presentations on this invisible potential foe inside neurons.
A Mouse Whose Neurons Perish in Droves
A vexing shortcoming of most mouse lines based on the amyloid hypothesis has long been that they do not show the massive neurodegeneration that marks the human disease they are made to model. Explanations abound (“mice are different,” “they don’t live long enough,” “they lack a tau component”), and neurodegeneration has even been made to seem secondary as the field shifted its focus on synaptic dysfunction, which existing mouse models do display to a small degree. But this smacks a bit of changing the topic. Even after years of recording LTP deficits and subtle behavioral phenotypes in the existing lines, critics of the amyloid hypothesis persistently point to the conspicuous absence of neurodegeneration from most models. Laurent Pradier of Aventis Pharma in Paris, with Thomas Bayer at Saarland University in Homburg, Germany, and colleagues, have given amyloid aficionados what they need—but with a twist.
In a pre-meeting symposium sponsored by the Alzheimer Research Consortium, and again at the conference, Pradier and Bayer presented a mouse line that develops dramatic neurodegeneration in the hippocampus. The point that generated the buzz is that these mice accumulate Aβ42 extensively inside their neurons, and that their neurodegeneration appears tied to this early form of Aβ42, not to the extracellular amyloid pathology that also develops in the mice.
The Franco-German team placed two familial AD mutations into the mouse presenilin gene and bred the resulting PS1 knockin mouse to the transgenic APP751 mouse. These APP751/PS1KI mice produce almost exclusively Aβ42, the most aggregation-prone form of the peptide. Normally, Aβ42 is a minor product of APP processing, and in some other APP/PS mouse models the ratio of Aβ42 to total Aβ increases but remains below 0.5. In this new line, this ratio exceeds 0.85.
Remarkably, the mice begin losing large numbers of pyramidal neurons in the CA 1/2 region of the hippocampus at six months of age, and this happens in parenchymal areas that have no plaques. The scientists also detected Aβ inside such neurons beginning at two months of age. The intraneuronal Aβ42 appeared to be aggregated, as thioflavin S, a marker of amyloid, produced granular staining.
“We think the intraneuronal Aβ42 leads to the death of neurons, not the plaques,” Pradier said. This would make Alzheimer’s more similar to other neurodegenerative diseases, where the protein accumulates to toxic levels inside neurons, for example, Parkinson’s (a-synuclein), prion diseases, and Huntington’s. It would also create a renewed sense of urgency about clarifying how Aβ and tau interact.
Presenilin Dysfunction: Not a Fringe View Anymore
One of the intriguing tie-ins of this work is how it dovetails with another recent study suggesting that some human presenilin mutations exert their effect through a partial loss of function (Saura et al., 2004.) Pradier and colleagues found that the APP CTF fragment that is the substrate for γ-secretase accumulates in their APP/PS KI mice, suggesting that the enzyme complex is partially inhibited. The hypothesis is that presenilin does not function properly, but what function it does have shifts the ratio of Aβ forms toward a relative increase in Aβ42. This idea would also explain the odd finding that, at low doses, some γ-secretase inhibitors actually increase the production of Aβ42, while at higher doses they shut down the enzyme complex. With regard to γ-secretase inhibitor drugs, Pradier said his data suggest that one needs a subtle modulator that nudges the enzyme complex away from producing Aβ42. In the context of presenilin dysfunction, it is interesting to note Bart Dermaut and Samir Kumar-Singh’s presentations on a PS1 mutation that leads to a splicing error and causes a tauopathy with intraneuronal Aβ but no plaques (see ARF related Philadelphia story).
Broadly, all this fits with earlier observations by Iva Greenwald, Ralf Baumeister, Christian Haass, Bart de Strooper, and others. These groups over the years all have found that some FAD PS mutants cannot reconstitute γ-secretase activity in C. elegans, yeast, and other systems. If such mutations acted strictly by a gain of function, they should be able to. In his presentation, Mark Fortini noted that some AD-relevant PS1 mutations act through partial loss of function. Nikolaos Robakis detailed in a plenary lecture the consequences for signal transduction and transcription of a loss of presenilin function caused by some FAD mutations, though he focused on pathways independent of Aβ.
The presenilin loss-of-function idea appears to become more widely accepted, but exactly how it relates to a role for intracellular Aβ is less clear. Pradier noted that this loss of function became apparent in his latest mouse strain because he kept the expression of the knockin PS1 gene at physiological levels. Generally, human transgenes are overexpressed, which can mask a subtle loss of function.
Not a New Idea, Just an Unloved One
Pradier’s and Bayer’s study gives a boost to those in the field who for years have been making a case for the role of intracellular Aβ. As early as 1985, Colin Masters and Konrad Beyreuther had written that “the amyloid is first deposited in the neuron, and later in the extracellular space.” (See Masters et al., 1985.) Eight years later, Virginia Lee, of the University of Pennsylvania, Philadelphia, demonstrated intraneuronal Aβ (Wertkin et al., 1993). Yesterday at the conference, Lee suggested in a lecture that different pools of Aβ exist inside neurons. One gets made in the trans- Golgi network and en route to nerve terminals, where it is secreted, she said. A second pool, however, accumulates over time inside the neuron. Lee hypothesized that this Aβ is actually made by a different γ-secretase, not the known complex containing presenilin.
What brought intracellular Aβ to the fore in this mouse model? The whole trick lay in shifting Aβ production toward the 42 variety, Pradier said, because this produced so much intraneuronal Aβ42 that it began aggregating to the point where thioflavin S picked it up.
Researchers have on occasion reported intraneuronal Aβ in human AD cases but, generally speaking, detecting it has been difficult. In Philadelphia, Charles Duyckaerts of Inserm in Paris, demonstrated intraneuronal Aβ with electron microscopy. Many labs have tried to do this, but few were able to. This French group met success by adding the Aβ antibody to brain sections of APP- and APP/PS1-transgenic mice, then fixing the sections and applying the secondary antibody with gold particles afterwards (gold is visible in the EM). Duyckaerts found that the Aβ42 accumulated within multi-vesicular bodies inside neurons, which also contained the lysosomal marker cathepsin D. This confirms an earlier finding by Gunnar Gouras, whose previous description of EM-immunogold localization of intraneuronal Aβ in mouse and human brain showed that it accumulated with age in the membranes of multi-vesicular bodies (Takahashi et al., 2002; Takahashi et al., 2004; ARF Live Discussion). Pradier’s group, too, has repeatedly described intraneuronal Aβ in mice (e.g., Wirths et al., 2001). But, like Gouras’s, it was not thioflavin-positive, nor was there massive neurodegeneration.
Changiz Geula, of Beth Israel Deaconess Medical Center in Boston, was intrigued enough by this evolving topic to look for intraneuronal Aβ in the brains of a group of primates he has been studying carefully for years. He looked for intraneuronal Ab accumulation in aged monkey brains, non-demented human brains, and four AD brains, and compared that with young monkey and human brains. In Philadelphia, he told his colleagues that he indeed found Aβ accumulation in hippocampal pyramidal and non-pyramidal neurons of old rhesus monkeys. He also found it in basal forebrain cholinergic neurons, which die early in AD, but much less so in other brain areas. Young rhesus monkeys and young human brains did not have this staining, but the brains of the AD patients did.
Not all postmortem studies jibe with this, however. Jerzy Wegiel’s group at the New York State Institute for Basic Research in Developmental Disabilities, Staten Island, reported that intraneuronal Aβ detection in control, Down’s, and AD cases argues against a role for it in AD pathogenesis. These scientists found Aβ inside neurons of infants and young people as well as people with AD. They suggest that, per se, intraneuronal Aβ expression is not related to neuronal death or neurofibrillary pathology. Other scientists cautioned in general terms that it is notoriously difficult to ensure that an antibody thought to bind AAβ inside neurons doesn't also recognize the Abeta sequence within APP.
How Do the Neurons Die?
On this question, Pradier would only reveal that the process differs from apoptosis, as the researchers looked for caspase activation but did not see it. He pointed out, however, that this mouse can be used to test neuroprotective agents directly in vivo, which is not possible with standard models of amyloidosis.
And how does this relate to tau? After all, neurofibrillary pathology is tied to neurodegeneration. In his mice, hippocampal and cortical neurons die without tau pathology, but the mice constitute an aggressive and artificial model, Pradier cautioned. In Alzheimer’s disease, it is more likely that an age-related build-up of tau pathology inside neurons sensitizes them, and that added Aβ42 accumulation pushes them over the edge, Pradier speculated.
By this hypothesis, plaques would remain behind after neurons have died. In fact, the death of a neuron could release pre-aggregated Aβ, which could perhaps act as a seed to accelerate the aggregation of extracellular Aβ into plaques. Plaques would then trap other proteins into binding to them and exert secondary toxicities in their own right, such as distorting neurites, Pradier said.
The question of whether direct links tie together Aβ—both inside and outside of neurons—and tau is still a nebulous one. The vapors appeared to lift a bit with Frank LaFerla’s presentation on what happens in his group’s triple transgenic mice (Oddo et al., 2003) after they receive shots of anti-Aβ antibodies into their hippocampus. In brief, the scientists showed that following treatment, the extracellular amyloid deposits disappeared first, then intraneuronal Aβ diminished and, a few days later, tau pathology vanished, as well. A month after the injection, amyloid pathology reappeared, followed by tau pathology. To LaFerla’s mind, this relationship between amyloid and tau pathology means that amyloid-removing therapies might indeed clear both amyloid and tau pathologies, but only if given before tau pathology has matured. This was also the conclusion of a plenary lecture delivered by Karen Hsiao Ashe. LaFerla’s work is slated to appear as the cover article in Neuron on August 5, when Alzforum will report on it separately in greater detail.
There were yet more presentations in support of the idea that intraneuronal Aβ figures prominently in the development of Alzheimer’s. They include recent work on the arctic mutation presented by members of Lars Lannfelt’s team at the University of Uppsala in Sweden. This group had discovered a family with early onset AD in Northern Sweden, whose APP mutation resides inside the actual Aβ sequence and makes the peptide more prone to aggregate. It appeared to point to a role of Aβ oligomers and protofibrils in driving disease (Nilsberth et al., 2001). In Philadelphia, Lars Nilsson presented data suggesting that combined SwedishArcticAPP-transgenic mice accumulate Aβ42 and form protofibrils and fibrils inside neurons. And Charlotte Stenh, also in Lannfelt’s group, said that previous, and puzzling, reports of a decrease in Aβ42 with this mutation were wrong because arctic Aβ42 aggregates so quickly that traditional ELISA tests do not quantify it correctly. That is because ELISA tests do not disaggregate protofibrils to record a signal from each Aβ unit. Denaturing the protofibrils first and then using antibodies against monomeric Aβ units gives a more precise measurement, and this method revealed increased levels of this peptide both extra- and intraneuronally, Stenh said.
What, then, does Aβ do inside the neurons? On this question, Claudio Cuello, of McGill University in Montreal, presented new data in support of the idea that physiological levels of it play a role in synaptic plasticity via a modest activation of CREB-directed gene expression. A pathological increase in intraneuronal Aβ would cause abnormal phosphorylation patterns that end up dysregulating these pathways. Cuello described work in transgenic rats that express intraneuronal Aβ in pyramidal neurons of the hippocampus and neocortex, as well as cell-culture work (see, for example, Echevarria et al., 2004). His research suggests that accumulating Aβ causes an upregulation of ERK, and that this kinase then phosphorylates a number of proteins, including tau. In t his way, this study suggests a further link between Aβ and tau pathways. ERK frequently pops up in gene expression comparisons between APP-transgenic and wild-type mice.
Cuello also told the audience that when intraneuronal Aβ levels rose in the rats, CREB phosphorylation diminished, uncoupling it from its normal function in regulating the expression of certain genes. CREB-driven gene expression has been found to be important for learning and memory; Cuello’s rats tested poorly in the water maze. Exploring this idea further in PC12 cells, the scientists found that CREB-driven gene expression depended on Aβ levels, but not on AICD. (AICD has drawn interest for its possible role in AD-related gene expression. But in Philadelphia, Thomas Südhof presented data suggesting that AICD may not do so itself, but merely induce a conformational change in the protein Fe65, readying it for its own gene regulatory function.) Cuello identified the Rap1/B-raf/MEK/ERK2 pathway as key to Aβ function, and said that it can become dysregulated by high concentrations of both intraneuronal and extraneuronal forms of the offending peptide.
To be sure, a great burden of proof remains before the field at large will be persuaded that intraneuronal Aβ accumulation damages neurons in early Alzheimer’s. But the idea is not languishing in obscurity any more. “Back in 1998, when I first presented data on intraneuronal Aβ at this conference, barely anyone paid attention,” Gouras remembered. At least that is no longer the problem.—Gabrielle Strobel.
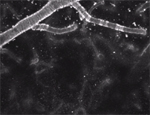





Comments
No Available Comments
Make a Comment
To make a comment you must login or register.