Tufted astrocytes? Astrocytic plaques? These tau pathologies mark progressive supranuclear palsy and corticobasal degeneration, respectively. The science of these difficult-to-diagnose diseases may finally be taking off. Read Tom Fagan’s coverage of the first PSP & CBD International Research Symposium held in London. Learn how genetics are yielding clues toward pathways, and natural history cohorts and therapeutic trials are getting underway.
International Symposium Puts PSP/CBD on the Map
Progressive supranuclear palsy and corticobasal degeneration are rare, poorly understood tauopathies with a broad array of symptoms and subtypes. What causes them? How to prevent, diagnose, track, and treat them? On October 25 and 26, 220 scientists gathered at the Royal College of Physicians in London to tackle these questions. Organized by Alex Klein of CurePSP in New York and Kate Arkell of the PSPA in Milton Keynes, U.K., the first PSP & CBD International Research Symposium drew researchers from fields of basic science to neuropathology. The meeting was opened by the Duchess of Gloucester, a longtime patron of PSPA.
The meeting marked a coming together of minds and gave these rare diseases their own voice in the dementia and movement disorders community. “Just a few years back we’d have been lucky to get 15 people at a PSP meeting,” said John Hardy, University College London. Klein noted, “It was exciting to have key opinion leaders of the field so focused on PSP/CBD, which often gets drowned out by discussion of more common dementias, such as Alzheimer’s.” Jeff Friedman, who is on the board of CurePSP and manages the PSP Genetics Consortium, agreed. “The quality of the science and the collaborative nature of the meeting showed how dynamic the field has become. It was encouraging,” he told Alzforum.
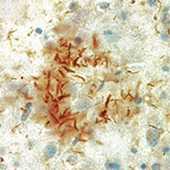
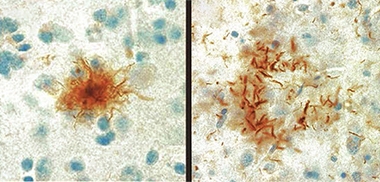
Tufts and Plaques.
Astrocytic tufts (left) and astrocytic plaques (right) of tau, are the pathological hallmarks of PSP and CBD, respectively. [Courtesy of Ruth Lamb, University College London.]
PSP and CBD typically become symptomatic in a person’s early 60s. They can progress quite fast, leading to death within three to six years after diagnosis, or six to nine years after symptoms start. Symptoms are similar in PSP and CBD, making the diseases difficult to distinguish clinically. Patients typically have trouble controlling movement, speech, swallowing, vision, and thought processes. Memory and cognition are often affected.
Postmortem, PSP is marked by so-called tufted astrocytes, which are caused by intracellular accumulation of tau in the soma of these glia. CBD also has astrocytic tau aggregates, but these look morphologically different, sit near the cells’ end processes, and are called astrocytic plaques. Neurons in PSP and CBD can also accumulate tau. In CBD, tau aggregates tend to be in cortical areas and basal ganglia, whereas in PSP they are in the basal ganglia and midbrain. Physicians tend to mistake CBD in particular for Alzheimer’s disease, and amyloid PET or CSF testing is often needed to get the diagnosis right. Unlike frontotemporal dementia, no tau mutations have been linked to PSP/CBD. Both diseases are rare, affecting fewer than five people per 100,000.
Presenters used the London conference as an opportunity to review ongoing research efforts, from the basic biology of tau to immunotherapy trials, from PSP/CBD brain banks to patient registries, from imaging and fluid markers to genetics. The latter had new data on offer, as well.
Genetics Points Toward Pathways
Scientists are starting to tap into the genetic variants shared by people with PSP or CBD. The largest PSP genome-wide association study to date, led by Ulrich Müller at Germany’s Justus-Liebig University, Giessen, and Gerard Schellenberg at the University of Pennsylvania School of Medicine, Philadelphia, genotyped about 2,000 cases in two phases, each with 1,000 cases. First author Günter Höglinger and colleagues identified risk variants in the STX6, EIF2AK3, and MOBP genes, which encode syntaxin 6, eukaryotic translation initiation factor 2-a kinase, and myelin-associated oligodendrocyte basic protein. The GWAS also confirmed that loci near the MAPT gene for tau, including the known rs242557 single-nucleotide polymorphism (SNP), associate with PSP (Jun 2011 news on Höglinger et al., 2011).
A smaller CBD GWAS led by Schellenberg and Dennis Dickson at the Mayo Clinic in Jacksonville, Florida, genotyped 219 cases (Kouri et al., 2015). It bubbled up the same SNPs near MOBP (rs1768208) and tau (rs242557), plus variants near the long noncoding RNA gene KIF13B-1 (rs643472) and near SOS1 (rs963731). The latter encodes son of sevenless homologue 1, a potential tau phosphatase.
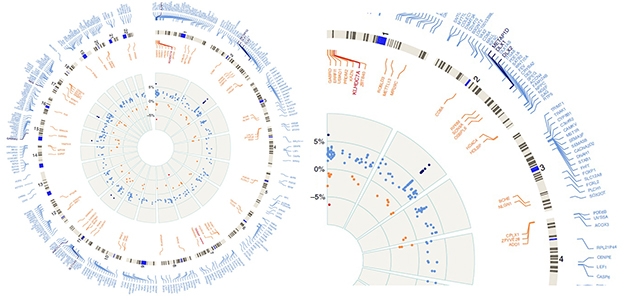
Epigenetic Changes. Circular plot, enlarged slice show hyper- (blue) and hypomethylated (red) regions of the whole genome by numbered chromosomes (outer gray circle). Inner gray circle represents percentage of up (to 5 percent) or down (to -5 percent) methylation relative to controls. The DLX1 locus on chromosome 2 is the most highly methylated in PSP, as represented by black dots on inner circle showing greater than 5 percent change in methylation status. [Courtesy of Günter Höglinger and Nature Communications.]
In London, researchers reported recent hits. Edwin Jabbari and Huw Morris at University College London took a phenotype approach to hunt for genetic variants that specifically associate with subtypes of PSP. They compared cases of Richardson syndrome against all other forms. This most common form of PSP was first described by Clifford Richardson at Sunnybrook Hospital in Toronto in 1955, with further cases identified by John Steele at the same institution (Steele et al., 1964). People with PSP-RS develop a rigid gaze, parkinsonian movement difficulties, and dementia. Because their eyes tend to be fixed straight ahead, people with PSP are prone to trip over pets, rugs, and furniture, putting them at great risk of falls. Their disease progresses more rapidly than non-Richardson PSP. It also has a higher tau pathology burden, especially in deep brain areas such as the subthalamic nucleus, globus pallidus, substantia nigra, and the pons.
Jabbari compared GWAS data from 367 PSP-RS cases to those of 130 non-RS cases. He found 27 SNPS, all in the q42.13 region of chromosome 1, and all inherited together, i.e., in linkage disequilibrium with each other. Of the 27, Jabbari believes rs564309 to be the lead candidate for a PSP variant. It lies between exons 3 and 4 of the gene for tripartite motif-containing protein 11 (TRIM11), which encodes a RING R3 ligase that activates the proteasome. Two of the other three genes residing in this locus are unlikely candidates for PSP genes, agreed Morris. One, obscurin, is expressed mainly in skeletal muscle, while Histone H3 is barely detectable in the brain. The fourth gene there, TRIM17, encodes another RING R3 ligase that shares 60 percent identity with TRIM11. Like its homolog, TRIM17 is expressed across the brain, and predominantly in the cerebellum. It is unclear which TRIM might be the link to PSP. It may be both, Morris said, since they seem to be co-regulated.
How do they increase risk? Jabbari suspects tau. He cited work suggesting that tau scuppers the 26S proteasome (Dec 2015 news), and said both TRIM 11 and 17 prime the proteasome to degrade proteins.
Deepening his confidence in a link between TRIMs and PSP-RS, Jabbari found variants that were in linkage disequilibrium with rs564309 in 100 well-characterized cases from Phase 1 of the Muller/Schellenberg GWAS. These findings appeared in the October Annals of Neurology (Jabbari et al., 2018).
Another potential risk variant emerged from whole-exome sequencing (WES). Schellenberg described WES data from 750 people with PSP. It identified the rs17662853 variant in the KANSL1 gene, which lies close to MAPT. KANSL1 encodes a component of a histone acetylation complex that regulates expression of up to 400 genes, said Schellenberg. A different mutation that introduces a premature stop codon in KANSL1 causes the neurodevelopmental cognition syndrome Koolen-de Vries.
Schellenberg has been unable to pinpoint how KANSL1 variants affect PSP, but is examining expression quantitative trait loci (eQTL) possibly regulated by the variant. Thousands of single-nucleotide polymorphisms in that region of the genome complicate the analysis. Schellenberg said KANSL1 SNPs don’t affect expression of tau, but might affect expression of nearby long noncoding RNAs. That would jibe with a recent report that PD variants in the MAPT region boost expression of transcribed non-coding elements, or TNEs, near KANSL1 (Oct 2018 news).
For his part, Höglinger investigates epigenetic regulation, which remains understudied in PSP. Samples of frontal cortices revealed 1,118 sites in the genome that are hypermethylated among 94 PSP patients relative to 88 controls. He also found 530 hypomethylated sites. Together, they cover some 450 protein-coding genes, but not MAPT.
The strongest signal came from a region encoding the DLX1 homeobox transcription factor. In PSP patients, this locus was highly methylated at multiple sites (see image above). This did not affect DLX1 expression but, lo and behold, reduced expression of a DLX1 antisense transcript. That, in turn, upregulated translation of DLX1. In keeping with this, the researchers found less DLX1AS in the brains of PSP patients relative to controls, and more DLX1 protein. Friedman complimented this approach. “It shows there are additional technical modalities we can use with existing sample sets, to pull out more data and identify potential targets,” he said.
What would having more DLX1 do? In neuroblastoma cells and Ntera-2 cells, which are an embryonal carcinoma line akin to neural precursors, Axel Weber and colleagues in Höglinger’s lab found that, at least in these cells, overexpressing the protein reduced tau levels. This is counterintuitive for a tauopathy. Höglinger thinks DLX1 may contribute to PSP by disrupting neuronal function. DLX1 appears to regulate tau expression indirectly by controlling expression of other genes, including those involved in Wnt and GABA signaling pathways. That might spell trouble for neurons. This work was published July 26 in Nature Communications.
Looking to future genetics studies, UCL’s Hardy called for more GWAS and challenged funders to support them. “Yes, maybe GWAS is so '90s and a bit boring, but we need more pieces to the jigsaw puzzle,” he said, referring to biological pathways that might be uncovered by new GWAS hits.
Taking his plea further, Hardy suggested that GWAS be done routinely and noncompetitively. This could be achieved by taking samples from all well-phenotyped cases as they come to clinics and running one large GWAS per year. “Since GWAS are now incredibly cheap, at about $60 a pop, they should be systematically run as samples are gathered by brain banks and even during clinical trials,” he said. Friedman agreed, saying the current GWAS are a good start but more are needed. Lawrence Golbe, Rutgers University, New Jersey, told Alzforum that Hardy’s idea holds merit provided the samples are well-characterized. “That could certainly work,” he said. “You’d have to get everybody to send their sample to a central lab and make sure the diagnostic quality was good. One thing that kills a GWAS is a few false positives.” On the up side, the positive predictive value for diagnosis of PSP-RS now exceeds 95 percent since clinicians have gotten adept at recognizing the disorder.
Meanwhile, the PSP Genetics Consortium plans to sequence at least 2,000 whole genomes. As outlined by Friedman, this project started as a collaboration among 11 investigators once they realized they had about 2,000 autopsy-verified cases between their groups, and another 100–200 accruing annually. Co-funded by CurePSP, the Tau Consortium, and NIH, and now expanded to 13 investigators, the project will sequence up to 3,000 PSP whole genomes and do GWAS on any new cases. Friedman hopes this work will find new risk alleles, targets, and pathways involved in pathology. It could also help stratify responders in clinical trials based on genotype, and identify protective alleles or mechanisms that delay disease onset. The project is committed to data sharing and joint analysis.—Tom Fagan
Höglinger GU, Melhem NM, Dickson DW, Sleiman PM, Wang LS, Klei L, Rademakers R, de Silva R, Litvan I, Riley DE, van Swieten JC, Heutink P, Wszolek ZK, Uitti RJ, Vandrovcova J, Hurtig HI, Gross RG, Maetzler W, Goldwurm S, Tolosa E, Borroni B, Pastor P, PSP Genetics Study Group, Cantwell LB, Han MR, Dillman A, van der Brug MP, Gibbs JR, Cookson MR, Hernandez DG, Singleton AB, Farrer MJ, Yu CE, Golbe LI, Revesz T, Hardy J, Lees AJ, Devlin B, Hakonarson H, Müller U, Schellenberg GD.
Identification of common variants influencing risk of the tauopathy progressive supranuclear palsy.
Nat Genet. 2011 Jun 19;43(7):699-705.
PubMed.
Kouri N, Ross OA, Dombroski B, Younkin CS, Serie DJ, Soto-Ortolaza A, Baker M, Finch NC, Yoon H, Kim J, Fujioka S, McLean CA, Ghetti B, Spina S, Cantwell LB, Farlow MR, Grafman J, Huey ED, Ryung Han M, Beecher S, Geller ET, Kretzschmar HA, Roeber S, Gearing M, Juncos JL, Vonsattel JP, Van Deerlin VM, Grossman M, Hurtig HI, Gross RG, Arnold SE, Trojanowski JQ, Lee VM, Wenning GK, White CL, Höglinger GU, Müller U, Devlin B, Golbe LI, Crook J, Parisi JE, Boeve BF, Josephs KA, Wszolek ZK, Uitti RJ, Graff-Radford NR, Litvan I, Younkin SG, Wang LS, Ertekin-Taner N, Rademakers R, Hakonarsen H, Schellenberg GD, Dickson DW.
Genome-wide association study of corticobasal degeneration identifies risk variants shared with progressive supranuclear palsy.
Nat Commun. 2015 Jun 16;6:7247.
PubMed.
Jabbari E, Woodside J, Tan MM, Shoai M, Pittman A, Ferrari R, Mok KY, Zhang D, Reynolds RH, de Silva R, Grimm MJ, Respondek G, Müller U, Al-Sarraj S, Gentleman SM, Lees AJ, Warner TT, Hardy J, Revesz T, Höglinger GU, Holton JL, Ryten M, Morris HR.
Variation at the TRIM11 locus modifies progressive supranuclear palsy phenotype.
Ann Neurol. 2018 Oct;84(4):485-496. Epub 2018 Sep 15
PubMed.
Can Clinical Trials and Longitudinal Studies Crack Rare Tauopathies?
When scientists gathered in London on October 25–26 for the first International Research Symposium on progressive supranuclear palsy and corticobasal degeneration, it was obvious that momentum was building in the study of these rare tauopathies (see Part 1 of this series). The change happened in large part because tau is now a tractable therapeutic target. Though PSP and CBD are often overshadowed by more common forms of dementia, such as Alzheimer’s, fledgling longitudinal cohorts and ongoing clinical trials are giving scientists tools to define and start to learn how to treat these disorders.
Researchers at the meeting were eager for any morsel of news on ongoing clinical trials; alas, there were no major announcements. Three tau immunotherapies are being tested for PSP/CBD. Tim Buchanan from UCB Pharma, Braine-l’Alleud, Belgium, reviewed the status of UCB0107, a humanized IgG4 that binds an epitope just before the first repeat in tau’s microtubule binding region. Two Phase 1 trials are underway in healthy volunteers, and a Phase 2 PSP trial is being planned.
Dosing in both Phase 1s, which tested up to 120 mg/Kg UCB0107 intravenously, is complete and the patients are being followed up. No clinically relevant safety issues have emerged to date, said Buchanan. He said the Phase 2 trial will be multinational, multicenter, randomize PSP patients to one year of drug or placebo, and measure change on the PSP Rating Scale. Buchanan said the design is not quite final, but the trial will begin in 2019.
Also a humanized IgG4 but binding the N-terminus of tau, ABBV-8E12 has appeared safe in initial Phase 1 trials and is being tested in the Phase 2 AWARE trial for AD (Aug 2017 conference news). Jorge Zamudio, AbbVie, Chicago, reviewed ARISE, a Phase 2 trial for PSP that is being run simultaneously with AWARE. It will test two doses against placebo for 52 weeks, and possibly a long-term extension. Patients must be 40 or older, have had symptoms for less than five years, and be able to walk at least five steps with minimal assistance. Recruitment is ongoing at 27 sites in the U.S. and another 27 sites worldwide, with expected enrollment totaling 330. So far, 233 patients have joined, Zamudio said. He showed their baseline data, suggesting they have similar characteristics to volunteers in previous PSP trials. As for UCB0107, the primary outcome is the PRPRS.
Another IgG4 that binds N-terminal tau, BIIB092, was developed to block spread of tau toxicity in the brain. It recognizes tau fragments released from human neurons. Tien Dam from Biogen, Boston, outlined safety data from an extension to a Phase 1 PSP safety trial run by Bristol-Myers Squibb, which sold rights to the drug to Biogen (Dec 2017 conference news).
The Phase 1 extension recruited 47 PSP patients who continued on their original dose of 150, 700, or 2,100 mg once a month. Dosing was staggered so that people on higher doses started later. By 48 weeks, 13 of the patients had discontinued treatment. Some withdrew consent, others dropped out due to adverse events or because their disease had gotten worse, or they no longer met eligibility criteria. The most common adverse events were falls, contusions, urinary tract infections, cough, and headache; these may be unrelated to the treatment, said Dam. Nine people had a serious adverse event.
Dam also mentioned the Phase 2 safety trial PASSPORT. In this one-year study with open-label extension, 234 of a planned 396 people have enrolled. They average 69 years old, have had symptoms for about 3.5 years, and have clinical characteristics similar to PSP patients from prior trials, Dam said.
In his overview of PSP/CBD clinical trials, Adam Boxer, University of California, San Francisco, outlined a new “basket” trial of BIIB092. The term is borrowed from oncology, where people with different cancers but the same underlying etiology, for example a specific mutation in an oncogene, are lumped into one clinical trial “basket.” TauBasket, primarily a safety trial, will include people with CBD, traumatic encephalopathy syndromes (TES), non-fluent variant primary progressive aphasia, or FTD due to tau mutations. Thirty-two volunteers will be randomized 6:2 to immunotherapy or placebo for six months, and blood, CSF, and MRI biomarkers will be assessed besides clinical and safety measures. The trial has begun and is slated to complete by 2020.
The scientists in London were curious how the three antibodies compared. “Based on the structure of abnormal tau, are some of these antibodies more likely to work than others?” asked Jonathan Rohrer, UCL. Boxer agreed this was an important question. “Maybe it is a coincidence that Abbvie and Biogen’s antibodies bind very close on the N-terminus, but we don’t really know the toxic species of tau, and all these antibodies have efficacy in mice,” Boxer said. Whether that translates into the clinic remains to be seen.
Others worry that the therapies are being tried too late. “All these studies require participants to be already significantly impaired. Is this the right population to study?” asked an audience member. Dam and others agreed this is a limitation, but noted they are hamstrung by the disease itself. “We need to be sure these patients do have tau pathology, so it’s a risk recruiting these [specific] patients but it’s unavoidable,” she said. Neither tau PET tracers nor CSF tau tests that reliably identify early stage PSP/CBD are available yet. Jean-Christophe Corvol from Hôpital Pitié-Salpêtrière, Paris, urged the field to figure out how to move earlier in clinical trials. “I agree we need the specificity but also think we may be treating too late,” he said. Boxer agreed that more natural-history data is essential so earlier stages can be diagnosed.
As for non-immunotherapy approaches, Boxer outlined a small safety trial of salsalate and young human plasma for PSP. Salsalate blocks acetylation of tau, a post-translational modification previously linked to pathology, while young plasma has been shown to protect old mice from neurodegeneration. In an open-label trial slated for six months, 10 PSP patients took 1,500 mg salsalate twice a day, and five PSP patients received four units per month of plasma from men younger than 30. Patient demographics were similar to those from prior trials. One adverse event led to a person dropping out of the salsalate arm; the others had unchanged progression rates as judged by change from baseline on the PSP rating scale (PSPRS) or volumetric MRI of historical controls. The point, said Boxer, was that large data sets from prior studies can be used to help power smaller ones. Some scientists are concerned that because PSP and CBD are rare, it may be hard to find enough patients to fill all tau-based trials.
Registries and Brain Banks
Researchers are banking that ongoing observational studies will help them characterize the early stages of PSP/CBD and related tauopathies. Dianna Wheaton gave an update of the FTD Disorders Registry. Founded in 2015, this independent, grant-funded registry set out as both a web-based community for patients and family members and a portal for the research community (Apr 2016 conference news). Opened to the public in March 2016, the registry exceeded its initial enrollment goals within 24 hours, said Wheaton, and to date more than 1,900 have signed up.
The registry admits people with PSP/CBD as well as FTD. Based on an intake survey, 51 percent have behavioral-variant FTD, 8 percent have PSP-RS, and 4 percent have CBD/CBS. They are predominantly white, with only 4 percent Latino, 2 percent African-American, and 1 percent each Asian and Native American.
The registry has two formats. One serves to provide information, the other follows an IRB protocol for informed consent to establish a trial-ready cohort. It complies with HIPAA, and Wheaton said the registry is undergoing an audit to ensure it satisfies new EU privacy standards as well. Ninety-three percent of registrants, including patients, family members, and spouses, said they want to participate in research, but only 26 percent have done so as yet. Wheaton hopes the registry will raise awareness and facilitate collaboration with researchers.
Over in the U.K., the PROSPECT study is a combined cross-sectional and longitudinal study to gather extensive data on PSP/CBS patients. Over five years, the prospective arm will conduct biannual clinical and cognitive tests for the first three years, assess daily living/quality of life up to five years, collect blood, DNA, and cell lines at baseline, and give patients a baseline smell test since loss of sense of smell has been associated with early Parkinsonism. MRIs and lumbar puncture at zero and 12 months, and eye-movement tests every six months up to three years, are optional. Patients in the cross-sectional study are seen but once, when their medical records are reviewed. They donate a blood sample and answer a questionnaire about their daily living and quality of life. This cohort will support genetics studies and help researchers track disease progression and milestones through analysis of ongoing medical records.
John Woodside, University College London, reported that as of mid-October PROSPECT had recruited 725 participants, including 82 controls, 218 patients in the longitudinal, and 425 in the cross-sectional cohort. The goal is to improve diagnosis, understand PSP subtypes, and get a handle on disease progression, said Woodside. PROSPECT will bank tissue and establish a trial-ready cohort. The youngest patient is 42 years old, which is quite young for PSP/CBD and hopefully may help researchers understand the early disease stages. Historically in PSP, fast deterioration and lack of antecedent markers or familial mutations made finding early stage patients almost impossible.
Since PROSPECT began, in March 2015, 88 participants with PSP or CBD have died. Only 15 of them had donated their brains for autopsy. Of the 13 who were clinically diagnosed with PSP, one turned out to have had CBD, while one of the two clinically diagnosed CBD cases turned out to have had Alzheimer’s disease instead. Woodside said this highlights the likelihood of misdiagnosis, and importance of autopsy. He has begun to use the PROSPECT cohort to develop a staging scheme based on the PSP rating scale (PSPRS).
A similar European registry for CBD, using a nearly identical protocol, has recruited 161 patients at 20 sites to date. One hundred and eight have been assessed on the PSPRS, 26 have had 3T MRI scans; 30 had CSF Aβ and tau tests, and of these nine had a CSF Aβ/tau ratio indicative of AD. Those patients also scored higher on the PSPRS, suggesting predominantly cognitive rather than motor symptoms.
Gesine Respondek from the German Center for Neurodegeneration (DZNE) in Munich outlined DESCRIBE PSP. This German observational study traces the natural history of PSP by way of its clinical presentation, genotypes, and fluid and imaging markers. DESCRIBE PSP aims to validate the most recently revised PSP diagnostic criteria established by the Movement Disorder Society (Jul 2017 news).
Started in December 2015, DESCRIBE PSP has enrolled 176 people who met MDS PSP diagnostic criteria at around a dozen sites. Forty participants have already been followed for a year; 29 of those have donated CSF, which is optional, said Respondek. Participants complete a clinical battery every six to 12 months, and have MRI and tau PET scans at least once but ideally every year. At baseline, 67 percent were diagnosed with PSP-RS, 13 percent with PSP-Parkinsonism; the remainder had rare subtypes such as PSP with pure akinesia and gait freezing or PSP frontal, which predominantly affects the frontal cortex. One goal is to determine how often a variant PSP diagnosis changes to PSP-RS, or vice versa. Parallel DESCRIBE FTD, multiple-system atrophy, and ataxia studies are also ongoing at the DZNE.
In London, Respondek outlined a separate German study called ProPSP, run by the Deutsche Parkinson Gesellschaft, i.e. the country’s Society for Parkinson’s and movement disorders. Recruiting at different sites than DESCRIBE PSP, ProPSP routinely tests patients on clinical battery, measures brain volume by MRI, and assesses tau accumulation using the three different PET tracers AV-1451, PBB3, and PI-2620. The latter appears to bind better than other ligands to the form of tau found in PSP (Dec 2017 conference news). “With these two parallels studies, we will have comprehensive geographical coverage of PSP in Germany”, said Respondek.—Tom Fagan
Comments
No Available Comments
Make a Comment
To make a comment you must login or register.