At the International Symposium on ALS/MND in Orlando, Florida, scientists, neurologists, and people with ALS were excited to hear about clinical progress to treat motor-neuron disease. Attendees pondered the preliminary, but positive, results of gene therapy trials in spinal muscular atrophy—results that may open the door for similar gene therapy in ALS. They heard news of completed and ongoing trials of edaravone, a drug that may slow ALS in certain people, and about therapeutics that relieve distressing problems with speech and swallowing. Basic science also made a showing. A better understanding of how pathogenic proteins travel from cell to cell emerged, and researchers debuted new genetic variants to explain some inherited ALS risk.
Gene and Stem Cell Therapies Make Strong Showing at ALS/MND Meeting
More than 800 researchers, clinicians, and patients with ALS gathered in balmy Orlando, Florida, on December 11-13, for the 26th International Symposium on ALS/MND. Attendees felt a sense of urgency, but also hope—urgency because “time is not on our side,” pointed out Sally Light, chief executive of the Motor Neurone Disease Association in the United Kingdom, which organized the conference. She noted that in the United Kingdom alone, six people die of ALS every day. Yet thanks to the advances discussed at the meeting, including novel therapeutic approaches, identification of new disease genes, and a growing understanding of how pathogenic proteins move from cell to cell, attendees felt the field was making progress. “I am wildly more optimistic than I was 10 years ago,” commented Kevin Talbot of Oxford University in the United Kingdom, chair of the program committee.
That optimism was most evident at a gene therapy session, when Brian Kaspar of Nationwide Children’s Hospital in Columbus, Ohio, presented early results from a clinical trial. He treated babies with the most severe version of the motor neuron disease spinal muscular atrophy (SMA), which normally causes paralysis and death within two years of birth. Yet all of the babies in Kaspar’s trial—started in spring of 2014—remain alive and wriggling. He played videos of a baby girl, six months out from her treatment, who sat up straight without support, something untreated babies with SMA never achieve.
“These are early, Phase 1/2 clinical trials,” Kaspar cautioned. “We are certainly not claiming victory, but it is exciting.”
“I thought the preliminary Phase 1 data Kaspar showed looked very encouraging,” commented Adrian Krainer of Cold Spring Harbor Laboratory in New York, who did not participate in the work. “Larger, [placebo] controlled trials will be necessary later on to determine if there are statistically significant improvements, but it is nice to see that there have not been safety issues.” During the same session, Krainer presented an antisense oligonucleotide therapy for SMA, which has also benefited participants in ongoing trials. In a separate session, Clive Svendsen of the Cedars-Sinai Medical Center in Los Angeles described his work to link up gene therapy with another promising modern technique, stem cell treatment, for ALS. His trial starts in early 2016.
Delivery vehicle.
Scientists use adeno-associated viruses to carry genes into patients.
Gene Therapy for SMA
SMA, an autosomal recessive disease, results from missense or deletion mutations in the SMN1 gene, which codes for the survival of motor neuron protein. SMN processes mRNAs, and for unknown reasons motor neurons are particularly vulnerable when they contain two bad copies of the SMN1 gene. Once motor neurons die, muscles wither without stimulation, causing the atrophy for which the disease is named. People possess a second SMN gene, SMN2, but a single nucleotide difference from the SMN1 code leads predominantly to an alternative spliced form that lacks exon 7. This shorter isoform is unstable and rapidly degraded. Nonetheless, the little bit of full-length SMN protein produced by SMN2 can be enough to allow people with two mutated copies of SMN1 to survive. In fact, the disease has a spectrum of severity, based on how much SMN2 is expressed. Some SMN1 mutation carriers with the mildest version, type IV, show no symptoms until their 30s, but in its most severe and most common form, type I—with almost no backup SMN2 expression—the disease cripples infants.
For the clinical trial, Kaspar and colleagues employed the harmless adeno-associated virus AAV9 to deliver a pristine SMN1 gene to motor neurons. Different AAV types, with different capsid structure, target different cell types, and AAV9 is able to cross the blood-brain barrier and bind to cellular proteins that have galactose attached, attracting it to both motor neurons and astrocytes (Foust et al., 2009; Shen et al., 2011). While AAV9 preferentially transduces astrocytes in adult mice, in larger animals it targets motor neurons and oligodendrocytes as well, Kaspar said.
Once it finds its target cells, the virus slips its genetic material into the nucleus, where it remains as an extrachromosomal bit of DNA. That DNA persists, so theoretically one treatment should provide SMN protein for a lifetime. In a mouse model of severe SMA, this treatment preserved mobility and mice survived past 27 weeks, whereas untreated animals survived around two weeks (see Mar 2010 news).
Kaspar licensed the treatment to the gene therapy company AveXis Inc., which is collaborating with Nationwide Children’s on a trial sited at the hospital. The study will enroll up to 18 infants, nine months of age or younger. All participants must have SMA due to SMN1 mutations on both chromosomes, with symptoms starting before six months of age, and low muscle tone with delayed motor skills. They will receive the one-time treatment with AAV9 carrying the SMN1 gene as an intravenous infusion, over about an hour. All participants receive treatment; there is no placebo arm. However, the study will test three doses of the virus, starting low and increasing in later enrollees. The authors suspect higher doses may work better, perhaps by transducing more motor neurons, or possibly by increasing SMN1 expression in individual cells or infecting glia as well as motor neurons, said collaborator Kevin Foust of Ohio State University in Columbus.
At the lowest dose, three babies received 67 trillion virus particles per kilogram body weight. The scientists have FDA approval to try 200 trillion per kilogram in up to nine more babies, and the highest titer of 330 trillion in the final participants. The researchers mainly will be looking for any toxic effects of the treatment, but will also assess the age at which babies either die or require a ventilator to breathe. They will compare their results to the standard progression of severe SMA (Finkel et al, 2014). SMA studies often rely on death or the requirement of a ventilator to breathe as a combined endpoint. Ordinarily, half of these babies would die or require a ventilator to breathe by 10.5 months, Kaspar said, and 92 percent would die or require ventilation by 20 months. In addition, the trial assesses movement by a standard score, with items such as gripping the tester’s hand while being lifted into a sitting position (Glanzman et al., 2010). The trial is expected to finish in June of 2017.
In Orlando, Kaspar reviewed the data so far. Three patients have received the lowest dose of the virus, and seven more received the intermediate dose of about 200 trillion per kilogram. The researchers have not tried the highest dose yet. Babies tolerate the infusion while awake with no problems, Kaspar said. From April of 2014, when the first baby was enrolled, to September 30, the last point at which the data were logged, Kaspar said that no babies in the study have died or required ventilation. They also moved better than they did before gene therapy, and the ones who received the intermediate dose benefited more than those who received the low dose. Though infants with severe SMA never manage to sit up on their own, the girl in Kaspar’s video could. The trial will continue with up to eight more babies, including some at the highest viral dose.
SMN Backup Therapy
AAV gene therapy can deliver a working SMN1 gene, but what if people could make use of the SMN2 gene they already have? It shares 99 percent of the SMN1 nucleotide sequence. In coding regions, SMN2 differs from SMN1 by a single cytosine-to-thymine switch, which prevents exon 7 inclusion in most transcripts but does not change the amino acid code. Krainer sought to promote exon 7 inclusion to create full-length SMN2 protein. Because the thymine substitution reduces affinity for a splicing activator needed to retain exon 7 in the mRNA, Krainer thought if he blocked a splicing repressor that sits nearby, he might coax the splicesome to incorporate exon 7.
To do this, Krainer collaborated with Isis Pharmaceuticals of Carlsbad, California, to make antisense oligonucleotides (ASOs) specific for the repressor binding site. Normally, ASOs instigate destruction of their target mRNAs by RNase H. In this case, the scientists modified the oligonucleotide backbone so RNase H does not recognize it; it just sits inert on the mRNA. Simply by being there, the ASO blocks the splicing repressor. When the spliceosome processes SMN2 hnRNA, now missing both a splicing activator and a repressor, it should incorporate exon 7, the theory goes. In fact, in SMA model mice, the ASO bumps up exon 7 inclusion from 15 percent to more than 80 percent, and extends lifespan from 10 days to an average of eight months at the maximum dose the researchers have tried (see Mar 2011 news; Hua et al., 2010).
The treatment, first called ISIS-SMNRx and rechristened Nusinersen, is now wending its way through clinical testing, Kainer said. Because oligonucleotides usually do not cross the blood-brain barrier, physicians infuse the drug via lumbar puncture. The oligonucleotide disappears from cerebrospinal fluid with a half-life of four to six months, so the doctors infuse it at regular intervals—every six months in children, and every four months in infants since their disease is more severe. In 2014 Isis announced that in two open-label Phase 2 trials, one of infants and one of older children, the ASO improved movement scores and survival. At that time, 11 of 16 infants who had received three doses of Nusinersen were still alive, with an average age at death or ventilation of 16.3 months for those on a 6 mg dose and 13.8 months for those on a 12 mg dose, compared to 10.5 months in the natural history study of untreated babies. For 14 of the participants, their motor scores also rose compared to baseline assessments, with an average increase of 9.3 points out of a possible maximum score of 64. As Krainer reported in Orlando, a couple of those babies who died of pneumonia came to autopsy, and scientists observed more SMN RNA and protein in their nervous system tissues.
In a trial of older children with SMA type II or III, aged two to 12 years old, Isis provided multiple doses of 1-12 milligrams of Nusinersen to 56 children, it reported in 2014. These kids also got stronger, improving by 1.5 to 3.7 points, depending on dose, out of a maximum of 66 on an expanded version of the Hammersmith Functional Motor Scale. In Orlando, Krainer said that 30 children continue with the treatment on an open-label extension, so some have been receiving the therapy for nearly four years.
Now, the company is recruiting for two Phase 3 studies, one of 111 infants aged up to seven months, and one of 117 children, aged two-12 who have a later-onset form of the disease. In each study, two-thirds of participants will receive Nusinersen, while one-third will receive sham treatment. The studies, started in 2014, are expected to wrap up in mid 2017.
Researchers at the meeting were thrilled by the progress in treating SMA, and said it gave them hope for treating ALS. “SMA is a trailblazer here,” commented Talbot, who did not participate in either trial. “It is showing that genetic disorders are, in a sense, tractable.” Similar treatments for familial ALS are already in preclinical and early clinical testing (see also Nov 2014 conference news; Jun 2015 news; May 2013 news).
ALS to Follow?
Kaspar and colleagues have made progress in developing therapies to shut down expression of the mutant SOD1 gene, which is responsible for about 10 percent of familial ALS. He used AAV9 to deliver short, hairpin RNAs that silence SOD1 to the spinal cords of transgenic mice that model the disease. In mice carrying human SOD1-G93A, which normally die at around 19 weeks, a one-time treatment improved survival by up to seven weeks. In a milder model that expresses SOD1-G37R, the treatment extended the 13-month average survival by three months (see Sep 2013 news).
The AAV9 virus included a gene for green fluorescent protein to mark infected cells, making it unsuitable for use in people. Kaspar and collaborators are now testing a new version without GFP. In the severe mouse model, some animals have lived beyond six months after a single treatment delivered when they were a day old. “To see this G93A mouse live beyond 200 days is really shifting the curve on survival,” Kaspar said. If the treatment proves safe in mice and macaque monkeys, he hopes to move forward with clinical studies.
Talbot said researchers still have some work to do to perfect this approach, pointing out that in the animal models SOD1 expression dropped, but not down to zero. “If you have a small amount of misfolded SOD1 in the aging nervous system, I think that could trigger disease,” he said. Foust suggested that the treatment would probably not eliminate disease completely, but over time would reduce SOD1 aggregation and slow or halt its course.
Perfecting Transfection.
Scientists used AAV9 to deliver SOD1 antisense oligonucleotides and green fluorescent protein (brown) to the spinal cord of a mouse. [Courtesy of Sara Gombash Lampe, Ohio State University, Columbus.]
In the closing session of the meeting, Svendsen explained how he combines gene and stem cell therapies in one. He noted that though motor neurons can be created from induced pluripotent cells and transplanted into the spinal cord, those cells do not usually integrate into the neuromuscular networks or connect to muscles. Plus, they would likely be subject to the same degeneration that plagued the original motor neurons in the cord. Instead, Svendsen chose to transplant astrocytes derived from stem cells that have been genetically engineered to pump out glial-derived neurotrphic factor (GDNF) (Suzuki and Svendsen, 2008). GDNF promotes motor neuron and corticospinal neuron survival, but the protein cannot easily be delivered to the brain, Svendsen said. The transplanted cells give it a ride (Henderson et al., 1994).
In rats expressing SOD1-G93A, the transplanted astrocytes survived for up to 11 weeks and released GDNF (Klein et al., 2005). Motor neurons survived for longer, and while the rats still developed paralysis, the nerves responsible for breathing—whose demise usually causes death in people with ALS—worked better than in control animals (Nichols et al., 2013).
Svendsen plans to enroll 18 people with ALS in a Phase 1/2 trial. The trial will start with transplants to the lower spinal cord, but Svendsen suspects multiple implants along the cord may be necessary. It is hard to predict outcomes for people based on the rat work, Svendsen told Alzforum, because the rats develop a severe disease due to multiple copies of the SOD1 transgene. The transplants might only improve breathing, or they might reduce paralysis too, he speculated.
Neurosurgeons will choose one side of the spinal cord to implant, based on where they can more easily avoid blood vessels that zigzag across the cord, Svendsen said. Since the stem cells do not cross from one side of the spinal cord to the other, the unimplanted side will serve as a control. Only the surgeon will know which side received the astrocytes, leaving everyone else involved in the study blinded. ALS symptoms typically progress at similar rates in both legs, Svendsen said, so the researchers will be hoping for slowed progression on one side, using a chair-like device that measures muscle strength to monitor symptom spread (see Oct 2011 news). “If something is happening, we should be able to detect it,” Svendsen said. He told Alzforum that if the scientists do detect benefit, they will offer participants implants in the other side of their spinal cords as well. He expects to enroll the first participant in the two-year trial in March of 2016.—Amber Dance
Finkel RS, McDermott MP, Kaufmann P, Darras BT, Chung WK, Sproule DM, Kang PB, Foley AR, Yang ML, Martens WB, Oskoui M, Glanzman AM, Flickinger J, Montes J, Dunaway S, O'Hagen J, Quigley J, Riley S, Benton M, Ryan PA, Montgomery M, Marra J, Gooch C, De Vivo DC.
Observational study of spinal muscular atrophy type I and implications for clinical trials.
Neurology. 2014 Aug 26;83(9):810-7. Epub 2014 Jul 30
PubMed.
Help for Speech, Swallowing, and Salivation Problems in ALS
People with ALS now have more options to deal with a distressing set of symptoms called bulbar signs. These include difficulties with speech, swallowing, and salivation that result from neurodegeneration of the bulb-shaped brainstem. The brainstem gives rise to motor neurons controlling head, neck, and facial muscles. At the International ALS/MND Symposium December 11-13 in Orlando, Florida, scientists presented promising results from two clinical studies. Richard Smith of the Center for Neurologic Study in La Jolla, California, shared how a drug called AVP-923, trade named Nuedexta, improved bulbar symptoms compared to a placebo. Edward Kasarskis of the University of Kentucky in Lexington offered another option to deal with excess saliva. He reported that radiation therapy to fry salivary glands proved effective and, importantly, safe.
When ALS attacks the brainstem, it causes facial muscles such as the tongue to atrophy. A person’s speech becomes hoarse or wheezy, making him or her difficult to understand, and many patients lose the ability to speak altogether. It can become hard to swallow not only food but also saliva. That, combined with trouble holding one’s head up and mouth closed, often results in drooling, too, even though people with ALS do not make more saliva than others. People find this distressing, Kasarskis noted; they may have to use a bib. Plus, not swallowing one’s saliva means losing up to 1.5 liters of water a day, risking dehydration.
Smith found a potential solution to the three bulbar signs—speech, swallowing, and saliva—in a medication used to treat another symptom of brainstem motor neuron disease, pseudobulbar affect. This occurs in ALS and other conditions when the neural circuits that control emotional response break down. People laugh or cry involuntarily, sometimes even if they are not feeling amused or sad. Nuedexta was approved in 2010 to treat pseudobulbar symptoms (Cruz, 2013). The main ingredient is dextromethorphan, an activator of the sigma-1 receptor and antagonist of NMDA receptors. The same stuff is commonly added to cold medicine because it suppresses the brain pathways that trigger coughing. Nuedexta also contains quinidine, which slows breakdown of dextromethorphan so it remains active in the bloodstream. Scientists are also testing Nuedexta for agitation in people with Alzheimer’s disease (see Sep 2015 news).
Scientists are not sure how dextromethorphan works against pseudobulbar symptoms, but the sigma-1 receptor prevents protein aggregation in the endoplasmic reticulum, protecting cells from apoptosis due to protein stress. Mutations in the sigma-1 gene are implicated in both juvenile ALS and motor neuron disease associated with frontotemporal dementia (see Aug 2011 news; Luty et al., 2010).
Smith initially prescribed Nuedexta for people with ALS who had emotional symptoms. He noticed that they reported bulbar improvements, too. To assess this objectively, Smith and colleagues recruited 60 people with ALS for a Phase 2 trial. Half received Nuedexta for a month, and the other half placebo. Then, after a couple of weeks to allow any drug to leave their systems, participants switched to the other treatment arm for a second month.
To evaluate the drug, the researchers came up with a 21-item scale, the Center for Neurologic Study-Bulbar Function Scale, by which people with ALS could rate their bulbar symptoms. They specified how often they experienced items such as difficulty making themselves understood, indicating they had trouble speaking clearly. A person with no problems would score a 21, and the worst possible score was 105. On this subjective scale, people on Nuedexta averaged significantly better (54) than the placebo group (59).
The drug worked regardless of whether people had emotional symptoms. However, about a quarter of the participants did not respond to the drug. Smith was unsure why. He also does not know how Nuedexta worked against bulbar symptoms, though he suspects the benefits resulted from its action on sigma-1 receptors.
Merit Cudkowicz of Massachusetts General Hospital in Boston, a co-principal investigator on the study, was pleased to see positive results from an ALS trial, where good news is rare. Cudkowicz has already started prescribing Nuedexta for her patients with bulbar symptoms. She predicted it could benefit many more since most people with ALS develop bulbar problems sooner or later.
Richard Bedlack of the Duke ALS Clinic in Durham, North Carolina, said he also has started to prescribe Nuedexta to many more of his patients since learning about the trial results. “It is very exciting,” he said, noting that previously physicians had no treatments to relieve difficulty with speech and swallowing.
“These results are quite promising and deserve further research,” added Kasarskis. He focused his presentation on just one of those bulbar issues, salivation. Cudkowicz, who did not participate in Kasarskis’ study, said it can be one of the hardest ALS symptoms to treat. Usually, physicians prescribe anticholinergic drugs, but they do not work for everyone and can have unpleasant side effects such as dizziness and constipation. As a second option, doctors can inject botulinum toxin into the salivary gland. Both methods work by interfering with acetylcholine signaling at synapses in the glands. However, using too much of the botulinum toxin could make swallowing even more difficult, and Cudkowicz said doctors often under-dose for fear of that. The notion of using radiation therapy for excess salivation has been around for decades, but neurologists worried that it was irreversible, and that if it worked too well a person would have a perpetually dry mouth. Cudkowicz said she has only prescribed it once.
Kasarskis and colleagues dared to give it a go. In 2011, they reported on 10 people who received radiation therapy (Kasarskis et al., 2011); at the meeting, he presented retrospective data from a total of 32. In total, his clinic has treated about 50 people with radiation, he said. They signed on because the salivation bothered them, or anticholinergic medications had failed.
Radiologists focused an electron beam at the parotid salivary gland in just one side of the mouth, through the skin of the outer cheek, leaving the other gland alone. People who received the therapy noted less saliva flow within weeks. To measure salivation objectively, the researchers placed cotton wads in each person’s cheeks for five minutes. Participants found it more comfortable to do both cheeks at once. The scientists weighed the cotton before and after, to calculate saliva production. Before radiation treatment, the average person produced about 2.5 grams of saliva in five minutes. After treatment, this dropped to about half a gram. The benefit lasted for at least two years, Kasarskis said, leading him to postulate it was “probably permanent.”
Importantly, the treatment was safe. One person suffered a bit of reddening skin at the radiation site, but this was temporary. No one developed dry mouth. Some people were able to stop taking the anticholinergic drugs; others found the medication more effective after radiation therapy.
“I was impressed not only by how effective this is for drooling (a very common and difficult-to-treat problem), but also how safe,” commented Bedlack. “I do plan to start offering this to patients who do not have a good response to medications.” Cudkowicz said that based on Kasarskis’ results, she would consider radiation the second line of treatment for salivation problems, ahead of botulinum toxin.
Kasarskis noted that researchers still need to work out the ideal dosing schedule. The University of Kentucky center administers a total of 1,500 centigray—a measure of how much radiation matter absorbs—over three different days to minimize adverse reactions to the radiation, such as skin blistering or nausea. That dose is low in terms of traditional radiotherapy, but may not be the ideal approach, Kasarskis said.—Amber Dance
Edaravone, a medication that scrubs cells of toxic free radicals, may help a subset of people with amyotrophic lateral sclerosis. That was the upshot of a presentation at the International Symposium on ALS/MND, held December 11 to 13 in Orlando, Florida. Koji Abe of Okayama University in Japan described results from two Phase 3 trials. The first found no treatment benefit, but in the second, Abe and colleagues identified a subgroup of mildly symptomatic participants whose decline seemed to slow down on edaravone. This second trial, completed in 2014, led to regulatory approval in June of 2015 of edaravone intravenous infusions for ALS in Japan.
Dutch businessman Bernard Muller, who spoke at the meeting about his efforts to promote ALS research in the wake of his own diagnosis, said he hopes for a similar benefit from an oral formulation of edaravone that is being tested in Europe. Meeting attendees buzzed about an announcement on December 10, 2015, from Muller’s pharmaceutical company, Treeway, of positive Phase 1 results. Now, Treeway plans a Phase 2/3 study.
Brian Dickie of the Motor Neurone Disease Association in the U.K., which organized the conference, told Alzforum he felt “cautiously optimistic” about the “hints of efficacy” in the edaravone results.
Edaravone
Also called MCI 186, edaravone is a drug originally developed by Mitsubishi Pharma Corporation. It was approved in Japan for the treatment of stroke in 2002, and subsequently in China, and India, where generic versions of the drug also are available. Physicians prescribe it to clear away free radicals and protect neurons following cerebral infarcts. The small organic compound neutralizes lipid peroxyl radicals and peroxynitrite, preventing injury to blood vessels and neurons in the brain (Yoshida et al., 2006; Fujisawa et al., 2015).
At the conference, Abe described his work taking edaravone to Phase 3 in ALS. Starting with an open-label, Phase 2 study in 15 ALS patients, two weeks of daily infusions of 60 milligrams of edaravone repeated every month for six months seemed to slow the march of their symptoms as measured by the ALS-Functional Rating Scale. In the ALS-FRS, physicians score people on 12 categories such as speech, walking, and breathing. On average, the participants lost nearly five points on this 48-point scale in the six months leading up to the trial, versus two points during the six months they received edaravone. Moreover, the concentration of 3-nitrotyrosine, a marker for oxidative stress, in their cerebrospinal fluid dropped to nearly undetectable levels (Yoshino and Kumura, 2006).
Based on those preliminary results, Abe and colleagues started the first randomized, double-blind, placebo-controlled Phase 3 study (Abe et al., 2014). As he described at the meeting, the researchers recruited 205 volunteers who had fairly mild ALS and were living independently. All developed symptoms within three years before the study start, and scored 70 percent or higher on forced vital capacity, a measure of exhalation volume. All met standard criteria for the diagnosis of ALS (Brooks et al., 2000). Study physicians classified some as either clinically definite or clinically probable ALS, with symptoms of both upper and lower motor neuron degeneration in multiple body parts. Others fell into a category called clinically probable-laboratory supported ALS; this meant they had fewer clinical symptoms, such as problems only in one body part, but their ALS diagnosis was supported by laboratory tests such as electromyography or neuroimaging to eliminate other possible diagnoses.
The researchers monitored the volunteers for 12 weeks before starting the treatment. All participants lost one to four points on the ALS-FRS during that time, suggesting their ALS was getting worse and a potential treatment benefit would be measurable. In this study, 121 people received edaravone infusions, and 104 a placebo solution, over 24 weeks. Results were disappointing: On average both treatment and control groups lost about six points on the ALS-FRS (Abe et al., 2014).
Abe and colleagues wondered if a subgroup might have benefitted, since ALS researchers have recently begun to suspect that certain treatments will work only for specific groups of people. Re-analysis of the data uncovered a more mildly affected subgroup that had a “small but significant benefit” from the edaravone treatment, Abe told Alzforum. These people had definite or probable ALS based on clinical symptoms, but their disease had started two years or less before the trial and their forced vital capacity was still 80 percent or higher. They scored at least two points in each of the 12 ALS-FRS categories, indicating they had not completely lost any one function.
People with clinically definite or probable ALS who had had ALS for longer and had lower lung capacity reaped no benefit from edaravone. Curiously, the ostensibly mildest subgroup—people with the clinically probable laboratory-supported diagnosis—did not benefit either. Researchers at the meeting had no explanation for why only some patients responded.
The Japanese researchers initiated a new Phase 3 trial focusing on people who did benefit, namely those with clinically probable or definite ALS, forced vital capacity of 80 percent or higher, and at most two years of ALS duration. Dickie and other researchers at the meeting praised the Japanese scientists for not simply trusting the post-hoc analysis, but testing that subgroup again. This time Abe and colleagues recruited 137 people, splitting them between treatment and placebo arms. Over 24 weeks, those on edaravone lost five points on the ALS-FRS, compared to 7.5 in the placebo group, a statistically significant difference, Abe reported. The authors are continuing to monitor edaravone’s effects in a post-market survey now that it has been approved in Japan. It should reveal whether edaravone can prolong life, Abe said.
Robert Miller of the Forbes Norris MDA/ALS Research Center in San Francisco commented that the subgroup Abe described seemed rather odd—its subjects' disease was mild enough that they could live on their own, but had progressed far enough to achieve a high level of diagnostic certainty. They might be people with fast-progressing disease, Miller speculated in an email to Alzforum, or people with a particular version of the disease that spreads to multiple body parts early on.
The efficacy in this subgroup suggests that early treatment will be most beneficial, he said. “Ideally, a longer study that would include survival would be highly desirable,” Miller said. “However, ALS is a terrible disease and these results are to me quite convincing of a beneficial effect on disease progression.” Nonetheless, he worried about the cost and logistics of a treatment that requires repeated infusions.
Muller hopes to solve that exact problem. Muller first heard about edaravone on a trip to Japan, as he described in the final session of the meeting. His company, Treeway, is pursuing an oral version of the drug, which would be more convenient for chronic treatment of ALS. (People who receive edaravone after stroke only need it for two weeks.) In two Phase 1 studies, Treeway administered multiple doses of the oral formulation to healthy volunteers, and single doses to people with ALS, Treeway CEO Inez de Greef told Alzforum. The drug seemed safe and well-tolerated, according to a company press release. While Treeway provided no data to directly compare with the intravenous formulation, de Greef said that adequate amounts of the oral drug entered the blood. The company plans to start a Phase 2/3 trial in 2016. It will run for at least a year, de Greef said, and include survival as an outcome.
Muller received a standing ovation after describing how his ALS diagnosis led him to apply his business skills to fundraising and research. His other projects include the worldwide sequencing initiative Project MinE, which Muller said currently stands at 7,000 ALS genomes (see Jul 2015 news). He called for more collaboration between patients and drug developers to speed up the time between a drug concept and its approval. “The patient’s voice should always be embedded in the process,” he said.—Amber Dance
SOD1, Tau Swept Up in Prion-like Biology at ALS Meeting
The first outward sign of amyotrophic lateral sclerosis (ALS) usually crops up in one spot: a little trouble swallowing, or weakness in one leg or one arm. Then it spreads. Scientists now suspect the underlying pathogenic proteins, such as SOD1, might pave the way for this symptom spread in prion-like fashion, traveling from neuron to neuron and converting good protein to bad. This was a major theme at the International Symposium on ALS/MND held December 11-13 in Orlando, Florida. Adopting injection seeding paradigms that have long been used in prion research, researchers find parallels between the structural variants of proteins involved in neurodegeneration, such as SOD1 and tau, and the “strains” of varying pathogenicity in prion biology. Importantly, scientists were not going so far as to call ALS a prion disease, according to Brian Dickie of the Motor Neurone Disease Association in the United Kingdom, which organized the conference. All the same, if ALS is driven by a prion-like mechanism, then treatments should be able to halt its progression, he speculated. Some speakers offered preliminary ideas about how to find and test such therapeutics.
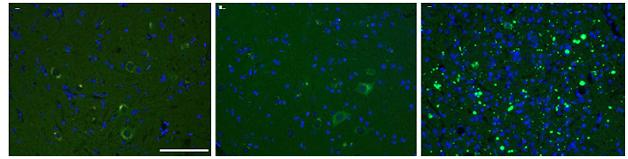
Pass it on. SOD1 aggregates in mice injected with tissue homogenates containing the SOD1-G93A “strain” (right), but not buffer (left) or homogenates from SOD1-G85R mice (center). [Courtesy of Acta Neuropathologica/Springer (Jan 2016, Vol 131, Issue 1, pp 103-114).]
SOD1 Gets a Move On Jacob Ayers of the University of Florida in Gainesville described strain-like properties of SOD1 he discovered during his efforts to follow SOD1 transmission in vivo (Ayers et al., 2014). As models, he used mice heterozygous for the ALS-associated human SOD1 variant G85R. He tracked a version of SOD1 G85R fused to yellow fluorescent protein (YFP) to see if the protein aggregated in vivo (see Jan 2009 news). These heterozygous mice do not develop motor neuron disease on their own. However, their genotype somehow made them vulnerable to the spread of toxic forms of SOD triggered by seeding injection experiments, compared to mice expressing only wild-type SOD1.
Ayers injected newborn mice intrathecally with spinal cord homogenate from paralyzed adult mice expressing toxic SOD1-G93A or G37R, two other ALS-linked variants. Six of 10 G85R mice injected with SOD1-G93A developed paralysis in their hind limbs between three and 11 months of age. Animal autopsy, aka necropsy, revealed punctate yellow SOD1 aggregates in the neurons of the spinal cord, brainstem, and thalamus. When Ayers injected homogenates from these animals into four new SOD1-G85R-YFP mice, disease occurred even sooner, with all animals developing movement difficulties within three months. In contrast, non-transgenic mice, or mice expressing wild-type human SOD1, that were injected with SOD1-G93A homogenates appeared normal, as did G85R-YFP animals injected with homogenates from non-transgenic mice.
The findings indicate that passaging toxic SOD1 variants through animals expressing G85R can convert this otherwise mild variant into a more pathogenic strain. That strain then more readily corrupts additional molecules of G85R SOD1.
This accelerated transmission in the second passage mimics the phenomenon of host adaptation seen in prion biology, in which the disease transmits more quickly between proteins identical in sequence, Ayers said (Aguzzi et al., 2007; Bruce et al., 1994). With prions, the concept usually refers to transfer between animals of the same versus different species; in this case it relates to the SOD1 genotype of the mice.
Ayers saw different results with the G37R and the G93A SOD1 variant. Even after more than 13 months, SOD1-G85R-YFP injected with homogenates from G37R animals developed no signs of motor neuron disease. In prion terms, SOD1-G93A and G37R would be considered different strains, Ayers pointed out.
In a study published last month, Ayers reported how SOD1 misfolding spread throughout the mouse’s nervous system following injection into the hind limb sciatic nerves of adult mice. In this case, he first injected homogenates from G93A mice intrathecally into SOD1-G85R heterozygotes. When these animals became paralyzed he used their tissue to make new homogenates that he injected directly into the sciatic nerves of a new batch of G85R mice. Aggregates appeared first in sensory neurons in the dorsal root ganglion on the injected side of the body, and from there spread to the contralateral dorsal root ganglion, spinal cord, and brain. In parallel, the mice lost strength first in the injected leg, then in the other. Within a month of the injection, both hind legs were paralyzed (Ayers et al., 2016).
The results represent a “grand slam,” commented Neil Cashman of the University of British Columbia in Vancouver, Canada, who did not participate in the project. “They have been able to develop a credible, in vivo model of SOD1-propagated misfolding, accompanied by paralysis,” Cashman said. SOD1-G85 seems to act as a sort of “acceptor” for SOD1-propagated misfolding in a way that the wild-type protein does not. Cashman speculated that in an aging person, wild-type SOD1 might become more prone to templated misfolding over time. This might be due to changes in proteostasis that leave it incompletely folded, or as a monomer instead of its natural dimer form, he theorized. This propagation contrasts the lack of pathology spread in other ALS models based on ubiquitous SOD1 transgene expression, Cashman noted. Ayers suggested that scientists could test therapeutics in mice injected with second-passage homogenates.
Edward Pokrishevsky, in Cashman’s group, also had therapeutics in mind. Pokrishevsky developed a high-throughput assay, based on the principles of toxic protein propagation described by Ayers, and used it to screen for possible blockers of SOD1 misfolding and propagation. In HEK293 cells, Pokrishevsky co-expressed SOD1-G85R tagged with green fluorescent protein (GFP), plus another more-toxic version of SOD1, such as the truncation mutant G127X. Alone, SOD1-G85R-GFP appeared diffuse, but in the presence of the second toxic SOD1 it aggregated in 20 percent to 30 percent of cells. Pokrishevsky reasoned that drugs that prevent SOD1 propagation should protect SOD1-G85R from aggregation, and could thus be identified in his assay
The researchers have not yet started a large screen, but Pokrishevsky presented uridine as a test case. He became interested in it because 5-fluorouridine (5-FU) binds to SOD1 at a tryptophan residue crucial for templated misfolding, suggesting it might block the conversion of new SOD1 molecules (see Oct 2011 news; Dec 2012 conference news; Wright et al., 2012). The Cashman lab found that 5-FU did indeed act in this manner. However, 5-FU is not a good therapeutic option for ALS because it can kill cells, said Pokrishevsky. It replaces uracil in DNA and RNA, blocking DNA and RNA synthesis, and also inhibits thymidylate synthase, disrupting production of thymine.
Because uridine has been used in people to counteract 5-FU toxicity, Pokrishevsky tested both together. The combination prevented SOD1-G85R-GFP aggregation. Surprisingly, so did uridine alone. Might uridine be a better drug candidate? Unfortunately, the dose needed was so high as to be impractical in vivo. Cashman told Alzforum his group plans to screen more molecules with Pokrishevsky’s assay this year.
The assay depends on mutant SOD1 to start and maintain propagation, but in other presentations Pokrishevsky and Cashman explained how wild-type SOD1 might also propagate as a prion. This may be important because SOD1 aggregates turn up in sporadic cases and in ALS caused by other mutations (see Oct 2010 news; Forsberg et al., 2010). The researchers wondered if variants of the ALS genes TDP-43 and FUS, or the cytoplasmic mislocalization of TDP-43 protein that marks nearly all human ALS, might lead to SOD1 misfolding and propagation. “Perhaps misfolded SOD1 is the common factor across all ALS,” Pokrishevsky told Alzforum.
If so, then conditioned media from HEK cultures expressing ALS-linked versions of TDP-43 or FUS ought to contain misfolded SOD1 that transmits its conformation to fresh cell cultures. Indeed, Pokrishevsky found that an antibody specific for misfolded SOD1 detected antigen in fresh recipient cells—either HEK cells or primary mouse neurons—but not if the antibody for misfolded SOD1 was first added to the conditioned media. Cashman concluded that once SOD1 has misfolded in one group of cells, it acquires the ability to transmit its altered conformation from cell to cell, like a prion. The lab is gearing up to test this idea in Pokrishevsky’s aggregation assay, Cashman told Alzforum. Notably, TDP-43 and FUS proteins in the recipient cells stayed where they were; they did not have to mislocalize or aggregate to support further SOD1 misfolding once it had started.
Ayers called the finding provocative, and noted it fits with Cashman’s previous work linking TDP-43 pathology and SOD1 misfolding in people with sporadic ALS (Pokrishevsky et al., 2012). Cashman speculated that treatment with the antibody to misfolded SOD1, or a therapy that knocks down normal SOD1 expression, could slow or halt ALS progression.
The Diversity of Tau Marc Diamond of the University of Texas Southwestern Medical Center in Dallas discussed different strains of tau. He noted that despite being based on just one protein, tauopathies manifest in myriad ways, ranging from Alzheimer’s and frontotemporal dementias and chronic traumatic encephalopathy to progressive supranuclear palsy and corticobasal degeneration. Different strains could explain both the progression of tau pathology across the brain and the diverse phenotypes, he reasoned.
In 2014, Diamond and colleagues reported their isolation of many different strains of tau. Studying two, they found that one produced large, cytoplasmic aggregates in cells and neurofibrillary tangles in mice. The other formed small, nuclear inclusions both in culture and the hippocampus. Importantly, as the researchers transferred brain material from affected to new mice, each strain maintained its phenotype (see May 2014 news).
In Orlando, Diamond reported his lab’s progress since then with similar characterization of 18 different strains of tau aggregates: eight from patient tissues, two from tau-P301S transgenic mice, and eight from recombinant tau fibrillized in vitro. The lab propagates them in cell cultures expressing tau. Since long-term expression of full-length tau can damage dividing cells, they use a HEK293 line expressing only the core part of tau that allows aggregation, amino acids 244-372, harboring V337M and P301L mutations and fused to YFP. The scientists originally chose this cell line because they thought it would be ideal to detect tau aggregates, Diamond told Alzforum. Disease-linked tau mutations usually make the protein more susceptible to prion conversion, he said, although wild-type tau can also be converted at a lower rate.
The strains had distinct identities. In cell culture, most were quite stable, displaying characteristic aggregates such as threadlike fibrils or punctate inclusions. Some aggregate types killed all the cells in a culture, while others killed only a subset. The deadliest strains were also the best at seeding new aggregates in cultured cells, Diamond said.
To study the structure of the strains, the researchers borrowed a technique from the prion world, using a protease to digest each strain. The protease completely degraded normal tau, but the aggregating strains yielded distinctive patterns of fragmentation depending on which portions of their structure were protected from digestion (see Aug 2013 conference news). These digestion patterns did not correlate in any way with toxicity or seeding ability, Diamond told Alzforum.
To learn what these tau strains might do in the brain, the scientists injected them into the hippocampi of transgenic mice expressing tau-P301S. They saw different patterns of pathology. For example, one strain remained in the hippocampus while another spread into the cortex. Some strains seeded widespread aggregation of endogenous tau within four weeks; others took a couple of months. The researchers noticed that the brain pathology did correlate with the protease digestion patterns, in that strains with similar digestion patterns had similar in vivo distributions.
Kevin Talbot of Oxford University in the United Kingdom, who led the meeting’s program committee, praised Diamond’s work, saying the different strains could explain how the same protein causes different diseases.
Unlike Ayers’ SOD1 mice, Diamond’s injected mice did not get sick within the two months the researchers have observed them thus far, he told Alzforum. He will monitor behavior and survival over longer time periods.
Dickie speculated that if ALS proteins do behave like prions, then future treatments could put up a sort of firewall to keep the problem isolated. In theory, this might limit symptoms to one body part and slow progression. Small molecules or antibodies might block the transit of prion-like proteins, Diamond suggested.—Amber Dance



Comments
No Available Comments
Make a Comment
To make a comment you must login or register.