Stress and Trauma: New Frontier Calling AD Researchers
( 6 Articles Available, 0 Articles Pending )
With the nation at war for eight continuous years, and awareness of the dangers of sports concussions on the rise, a new priority—and opportunity—are taking shape for neurodegenerative disease researchers. In a time of austere budgets, the Department of Defense last week allocated $15 million of new research funds for grants exploring Alzheimer's disease, chronic traumatic encephalopathy, and related conditions, particularly in veterans. Are veterans with blast trauma or post-traumatic stress disorder at higher risk of premature neurodegeneration, as is thought to be the case for some athletes prone to head injury?
Stress and Trauma: New Frontier Lures Alzheimer’s Researchers
As an army medic in Iraq, Specialist Kara Wooten was caught in the blast radius of improvised explosive devices six times. The first five rattled her brain but left her conscious; the last one knocked her out. Two months later, Wooten began to have severe headaches, muscle spasms, seizures, and lost her balance. Vision problems developed, as well as weakness on her left side. A history major in college, she soon struggled to speak, forgot common words, and had trouble remembering. She was diagnosed with traumatic brain injury caused by multiple mild concussions.
Wooten’s story appeared in the Santa Cruz Sentinel in 2008, but has become only more relevant since then. Wooten is one of an estimated 200,000 service members who have sustained brain injuries since the year 2000, according to statistics from the Defense and Veterans Brain Injury Center (see stats). That is about 10 percent of the roughly two million military personnel who have served in Iraq and Afghanistan. Her fate leads this series on Alzforum for two reasons. First, science is recognizing the scale of the problem and tackling its potential implications for premature dementia. Second, Veterans Affairs hospitals contacted by this reporter have been unwilling to make additional veterans available to tell their stories.
The wars of the last decade have highlighted the effects of traumatic brain injuries (TBIs) and post-traumatic stress disorder (PTSD), with hundreds of thousands of young people bringing home these invisible wounds of war. Science still does not understand all of the long-term consequences of the conditions, but a growing body of research suggests these injuries may hasten pathogenic processes that lead to dementia. Several scientists contacted by this reporter fear that young soldiers and athletes with brain injuries could be at risk for prematurely aged, degenerative brains. Worse, current treatment options for both disorders are limited to symptom management. To tackle the problem, organizations like the Department of Veterans Affairs are launching new initiatives that have lured Alzheimer’s researchers to study these issues. VA programs encourage scientists to focus on novel treatment strategies and explore the genetic underpinnings of susceptibility and recovery. Other agencies are sponsoring a TBI conference to be held this June to bring together civilian and military researchers to share the latest data in this field.
Most tellingly, the new budget passed by Congress 14 April 2011 includes $15 million to create an Alzheimer’s Research Grant Program within the Department of Defense. The research focus will include investigations into the links among Alzheimer’s disease (AD), TBI, and PTSD. This grant is all the more remarkable in an otherwise punishing budget climate where overall funding for the National Institutes of Health was cut (see ARF related news story, or a press release from USAgainstAlzheimer’s).
This series surveys current research, underscoring the many unanswered questions that remain. Part 2 will focus on severe brain injuries, which have been shown to spur Aβ peptide deposition and increase the risk of AD. In Part 3, the spotlight will shift to sports medicine, where the data show that athletes who suffer repeated mild concussions can develop a unique form of brain degeneration. Part 4 will look at emerging data from veterans who were exposed to multiple blasts. Neuroimaging from the brains of these young people shows patterns of degeneration typically seen in elderly people with mild cognitive impairment. Part 5 will cover the controversial link between PTSD and dementia and review conflicting data. The series will wrap up with a look at some of the initiatives to study PTSD and the efforts to find effective treatments.
Brain injuries are more prevalent in the current conflicts than in any previous war. Improvised explosive devices are in widespread use. Thanks to improved body armor, soldiers and marines now survive blasts that would once have killed them. The flip side of this advance is that more service members are walking away with invisible wounds, head injuries whose effects may not become apparent for weeks, months, even years. About three-quarters of these TBIs are classified as “mild,” meaning they involve only a brief period of disorientation or unconsciousness. Growing research indicates that repeated mild TBIs can have serious, long-lasting consequences on the brain, as they did for Wooten. The initial injury may go unnoticed and untreated, which means TBIs are often underdiagnosed. In a telephone survey of 2,000 returned service members, almost 20 percent reported experiencing a brain injury (see Stein and McAllister, 2009), twice the percentage that is officially diagnosed.
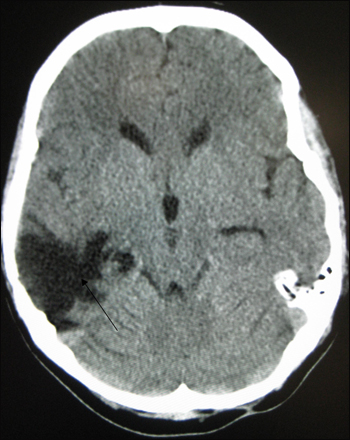
CT scan of severe traumatic brain injury shows long-lasting lesion. Image credit: James Heilman via Wikimedia
Elaine Peskind at the VA Puget Sound, Seattle, Washington, a noted Alzheimer’s researcher who studies brain trauma in veterans, believes that the number of military personnel affected by TBIs will go even higher as service members are repeatedly deployed. For example, in one U.S. Army brigade that served in Iraq, almost 23 percent of them were diagnosed with TBI (see Terrio et al., 2009). Peskind also notes that in her small study of 35 veterans with TBI, the men had been caught in an average of 16 blasts each. She predicts that this high frequency of exposure will become more common as deployments increase. Peskind’s neuroimaging data on young veterans are featured in Part 4 of this series.
Another invisible disorder that often goes along with TBI is post-traumatic stress disorder. PTSD is a cluster of anxiety-related symptoms that sometimes follow traumatic events. In surveys of service members returning from Iraq and Afghanistan, 8 to 16 percent of them admit to PTSD symptoms (see Milliken et al., 2007 and Smith et al., 2008), although the stigma attached to them makes it likely these symptoms are underreported (see Stein and McAllister, 2009). Since the types of events that cause traumatic brain injury also cause severe combat stress, the two conditions are often linked. Peskind estimates that in her studies, about three-quarters of the veterans with TBI also have PTSD, and vice versa.
Both TBI and PTSD involve changes in the brain. Neither condition is well understood yet, but research in these areas is heating up. Many scientists contacted for this article stressed that this is a field in its infancy. One of the biggest concerns is that in epidemiological studies, both TBI and PTSD have been linked to an increased risk of developing dementia (for details, see Part 2 and Part 5). The evidence for a causal role in dementia is stronger for TBI than for PTSD, but in neither case has such a link been conclusively proven.
The questions outweigh the answers right now, but there is a growing interest in research into these conditions. For example, the Third Federal Interagency Conference on Traumatic Brain Injury will take place 13-15 June 2011 in Washington, DC. The last such conference was in 2006. Talks run the gamut from the role of Aβ in TBI, to neuroimaging and biomarkers, with special emphasis on prevention, diagnosis, and treatment. In the amyloid session, Mark Burns, an AD researcher at Georgetown University in Washington, DC, will discuss evidence from animal models demonstrating that reducing Aβ levels can improve brain health after injury. His fellow presenters will talk about what happens to the Aβ that accumulates in damaged brain tissues, as well as the possibility of using Aβ as a biomarker for TBI, Burns wrote in an e-mail to ARF. “There has been growing interest in AD-related pathways both acutely and chronically after TBI,” Burns told ARF. “TBI is thought to be a risk factor for the development of AD in late life.” Another presenter, Milos Ikonomovic at the University of Pittsburgh, Pennsylvania, wrote to ARF: “It is now recognized that, similar to severe TBI, repetitive head injuries in high-contact sports and modern warfare can result in pathological and clinical changes characteristic of chronic neurodegenerative disorders including AD.”
Sam Gandy, at the Mount Sinai Medical Center in New York City, thinks it will take a concerted effort for scientists to get a handle on brain injuries. Pointing to the need for more data and larger brain banks, he suggests the TBI field could benefit from a network of nationwide research centers, similar to the Alzheimer’s Disease Research Centers, that could share resources. TBI is complex, Gandy told ARF, because it consists of several related disorders: single mild brain injuries; repeated concussions such as many athletes sustain; severe brain injuries; and military brain injuries caused by explosions, which may also involve PTSD. These probably all have distinct pathology and require different treatments, Gandy suggests (see DeKosky et al., 2010).
The evidence that brain injuries spur early degeneration, such as that suggested by Peskind’s VA-funded imaging studies on young veterans, is enough to concern researchers at the Department of Veterans Affairs. Tshaka Cunningham, who runs the research program on aging and neurodegenerative diseases at the VA, told ARF that the issue of increased dementia risk is on his radar, and with this comes funding opportunities for AD researchers. In 2005 the VA solicited research on Parkinson’s disease, Alzheimer’s disease, and other neurodegenerative disorders, and in 2008, it launched an initiative to promote research on traumatic brain injury. Cunningham said the VA encourages research proposals on AD, and particularly on potential treatments, anything from novel Aβ-lowering compounds to vitamin therapy.
“We are keen to understand if there are downstream consequences for these brain injuries,” Cunningham said. “We are trying to stimulate more research in the field on that exact problem.”
Additionally, the VA would like researchers to explore the contribution genes make to health disorders, and particularly to recovery. For example, what makes some people more resistant to PTSD, or allows them to bounce back faster from brain injury, than others? In January 2011, the VA launched the Million Veteran Program to try to pin down some of these genetic factors. The project will collect DNA as well as health and lifestyle information volunteered by veterans receiving care at VA centers nationwide. The VA expects to enroll one million veterans in the program over the next five to seven years, which will make this one of the largest such databases in the U.S. The data will be made available to VA researchers, federal health agencies, and U.S. universities for research projects that will look for patterns between specific genes and medical outcomes. Knowledge of which people are at greater risk for certain diseases might lead to more effective prevention, the VA suggests. The research could also produce treatments that are better targeted to an individual’s genetic makeup.
“Hopefully these new program announcements will spur the research,” Cunningham said. “We are encouraged by the increased number of applications, and we want to fund as much exciting new research for the benefit of our veterans as we can. I am hopeful that we will see some breakthroughs in the years to come.” For details on head injury, Aβ, and dementia, see Part 2.—Madolyn Bowman Rogers.
Stress and Trauma: Aβ’s Mysterious Role in Severe Brain Injury
Traumatic brain injury (TBI) has become a hot topic. Between the high number of military personnel exposed to blasts from homemade bombs and a new awareness of the seriousness of concussive sports injuries, the disorder has grabbed the attention of many researchers. One especially troubling question is whether brain injury seeds the development of dementia. The data to date are suggestive, but far from conclusive.
An important factor to keep in mind is the nature of the brain trauma. “We should not assume that the processes occurring after a single severe injury are identical to those occurring after repetitive concussive injuries,” said David Brody of Washington University in St. Louis, Missouri. Brody is currently comparing mouse models of each type of head trauma, and said that preliminary data suggest there are substantial differences between the two, although it is too early to give details. One feature shared in common is axonal injury—these long, thin nerve fiber tracts appear to be supremely vulnerable to shearing, stretching, and twisting damage (see Smith et al., 2003). Yet even for axons, Brody said, the exact nature of the injury may differ in severe versus mild TBI.
Aβ deposits (red) and APP (green) at a site of axonal injury in mouse brain. Image credit: David Brody and Hien Tran
Severe TBI has been better studied, with a more extensive literature. “Most of the evidence for increased risk of dementia of the Alzheimer’s type is after single severe injuries,” Brody points out (see, e.g., Mortimer et al., 1991; Jellinger et al., 2001; Jellinger et al., 2001; and Fleminger et al., 2003). In one study of almost 2,000 World War II veterans, those with moderate to severe head injuries had twice the risk of developing dementia, and for those with an ApoE4 allele, the risk seemed to increase further (see Plassman et al., 2000).
Numerous papers agree that ApoE4 increases TBI-related dementia risk (see, e.g., Isoniemi et al., 2006; Mauri et al., 2006; and Luukinen et al., 2008), with one influential study finding that people with head injuries had a 10-fold increase in AD risk if they also carried an ApoE4 allele (see Mayeux et al., 1995). The finding is not universal, with a few small or short-term studies showing no association (see, e.g., Chamelian et al., 2004 and Han et al., 2007). Overall, however, the data imply a role for AD-related processes after head injury.
Does the increased risk for AD mean that severe brain injury triggers Alzheimer’s pathology? Not necessarily, Brody said. Such injuries might merely lower a person’s overall brain health and cognitive reserve, leading to an earlier onset of AD symptoms later in life. Or some third factor could be at work. For example, a recent review posited that sleep apnea, which is common among TBI patients, may be a source of cognitive impairment and dementia risk after brain injury (see O’Hara et al., 2009). This idea would be encouraging, since sleep apnea is treatable.
Several studies do point to a possible link between severe brain injury and Alzheimer’s disease processes, however. In animal models, amyloid precursor protein (APP) accumulates in injured axons, where it may be snipped by β-secretase, presenilin-1, or caspase-3 to make Aβ (see Stone et al., 2002 and Chen et al., 2004). Inhibiting caspase-3 lowers Aβ levels after brain injury and improves recovery in mice (see Abrahamson et al., 2006). Likewise, administration of anti-APP antibody to rats with rattled brains reduces neuron and glia death and improves cognitive function (see Itoh et al., 2009 and Itoh et al., 2009). In a mouse study, inhibition of APP-cleaving β- and γ-secretases had similar beneficial effects (see ARF related news story on Loane et al., 2009). These findings suggest a role for amyloid pathology in the deficits caused by head injury, at least in animal models.
In humans, researchers have seen contradictory changes in the levels of Aβ40 and Aβ42 in cerebrospinal fluid after severe brain injury, with some studies showing an increase and some a decrease (see Emmerling et al., 2000; Franz et al., 2003; and Olsson et al., 2004). The literature on amyloid changes in the brain is also confusing. In about one-third of brain samples surgically removed within hours of severe TBI, researchers have found diffuse Aβ plaques (see Ikonomovic et al., 2004). TBI brains containing plaques also show higher levels of soluble Aβ42 (see DeKosky et al., 2007). Brody and collaborators measured levels of extracellular Aβ in brain interstitial fluid taken from drainage catheters of trauma patients in intensive care, however, and found peptide levels were lower after the brain injury, when the injured brain’s activity was low, and gradually rose as the brain recovered and resumed activity (see ARF related news story on Brody et al., 2008; Schwetye et al., 2010; and reviewed in Magnoni and Brody, 2010).
“It is possible that in humans with TBI, extracellular amyloid-β levels are reduced in the soluble form, yet intracellular amyloid-β levels are increased in an insoluble form,” Brody said, emphasizing that the brain contains different pools of Aβ. “That would fit with all the available animal and human literature.” He notes there is no data as yet on the oligomerization status of the soluble Aβ, a key factor for determining its toxicity.
Despite the research to date, it is not clear how injury-associated amyloid release relates to AD. Do diffuse post-injury deposits go on to seed Alzheimer’s-like plaques? At least one study that examined TBI patients surviving up to three years after injury suggests not, finding that, despite the presence of large amounts of APP and Aβ, there were “virtually no” Aβ plaques in these brains (see Chen et al., 2008). This would suggest that post-injury deposits may be a fleeting phenomenon that the brain subsequently clears. Likewise, at autopsy, only about one-third of people who have had severe brain trauma show amyloid deposits, Brody said.
Mark Burns, at Georgetown University in Washington, DC, wrote to ARF, “This leads to a very confusing picture of why the brain becomes susceptible to AD after TBI. I suspect the answer may be that the brain has suffered a severe stress that leaves it primed and vulnerable to other stressors as time progresses.” This might lead to an earlier onset of AD, Burns suggested.
However, Sam Gandy at Mount Sinai Medical Center in New York City told ARF that he is convinced by the data that Aβ42 accumulation triggered by brain injury does play a role in susceptibility to AD. Cognitive reserve may be lost as well, Gandy wrote, both through amyloid-related and non-amyloid pathways.
Brody points to the need for more standardized, validated animal models of brain injury to sort all this out. Such models are in development (see, e.g., Brody et al., 2007), but much more work will be needed to answer these questions. To find out what role tau plays in chronically concussed brains, see Part 3.—Madolyn Bowman Rogers.
Athletes who suffer repeated concussions in high-impact sports such as boxing, football, and hockey are at risk for long-term brain damage. Some of them develop a degenerative condition known as chronic traumatic encephalopathy (CTE), also called dementia pugilistica (see ARF Live Discussion and ARF related news story). The condition can occur even in relatively young athletes. Hockey player Bob Probert, who died this year of heart failure at the age of 45, was recently found at autopsy to have CTE (see March 2 New York Times story). Probert was known as an “enforcer” due to his aggressive play and frequent fighting. The findings are sobering, given that Probert played in the modern era of helmet use, unlike previous CTE cases seen in hockey players from earlier eras.
The scope of the problem is great. The CDC estimates that more than a million Americans are treated for mild or moderate brain injuries each year, and about 200,000 of these injuries are sports related (see Morbidity and Mortality Weekly Report, 2007). However, because only about 10 percent of head injuries lead to a hospital visit, the actual number of traumatic brain injuries (TBIs) may be 10 times greater than this, the CDC noted. Researchers do not know how many of these TBIs are repeat injuries that increase the odds of developing a chronic condition, nor do they know how many concussions a brain can take before suffering long-term damage.
Brains with mild TBI (top row) show a similar pattern of changes to MCI brains (bottom row) by PET scan.Image credit: Elaine Peskind
Ann McKee, an expert on the pathology of sports-related head trauma at the Bedford VA Medical Center, Massachusetts, and Boston University, has probably seen more CTE brains than anybody. She runs brain banks at Bedford, Boston University, and the Center for the Study of Traumatic Encephalopathy at Boston University, among others, and has examined dozens of brains with CTE. CTE is “a unique disorder that is clearly associated with mild repetitive head injury,” McKee said, adding that it is “quite unlike any neurodegenerative disease I have ever studied.”
The disorder is primarily marked by deposits of tau and TAR DNA binding protein 43 (TDP-43), McKee said. Only about 40 percent of CTE brains she has looked at have Aβ deposits, and even when they are there, the plaques are diffuse and the amyloid load is smaller than in AD patients. “Aβ is definitely a characteristic of acute traumatic brain injury, but it may not persist into the chronic state,” said McKee, suggesting that Aβ deposition may be a phase reaction that is later cleared. This is similar to data from studies of severe TBI, which suggest that in that condition as well, Aβ deposits may be transient.
TDP-43 deposits also characterize amyotrophic lateral sclerosis (ALS) and some forms of frontotemporal dementia (FTD), while tau tangles mark Alzheimer’s disease and other subclasses of FTD. The tau tangles in CTE show abnormal phosphorylation similar to those seen in AD (see Schmidt et al., 2001). Although CTE shares features with other neurodegenerative disorders such as Parkinson’s, AD, and ALS, McKee said its overall presentation is distinctive.
Henrik Zetterberg at Sahlgrenska University Hospital in Molndal, Sweden, agrees that repeated head trauma causes a specific disorder. “I believe repeated brain trauma is more related to subcortical axonal injury than to an Alzheimer’s disease process per se,” he said. For instance, in one study that analyzed the cerebrospinal fluid (CSF) of boxers immediately after a match, Zetterberg and colleagues found elevated levels of biomarkers that indicate axonal injury, such as neurofilament light protein and total tau, but they did not see Alzheimer’s-like changes in Aβ or phosphorylated tau levels (see Zetterberg et al., 2006).
“This pattern looks more like what we see in cerebrovascular disease,” Zetterberg said. Because the brain cells that are most sensitive to hypoxia are myelin-producing oligodendrocytes, Zetterberg said, cerebrovascular disease damages subcortical myelinated thick-caliber axons, which may be the same axons damaged by repetitive head trauma. These axons connect association areas in the cortex and other brain regions. The resulting disorder gives a different clinical picture from Alzheimer’s, Zetterberg said. “The symptomatology is more slowness of thought and slowness of movement, parkinsonism combined with memory or cognitive problems.” One example of this presentation would be the boxer Muhammad Ali, who developed Parkinson’s-like symptoms after many years of boxing.
Nonetheless, Aβ may be involved as well, Zetterberg said. “Some processes in AD are activated by brain trauma,” he said. “Close to an injured axon, you have increased processing of β amyloid precursor proteins, so that more β amyloid is formed.” For example, an animal model of repetitive mild TBI demonstrated increased brain Aβ levels along with cognitive impairment (see Uryu et al., 2002). Patients with diffuse axonal injury have higher levels of Aβ42 in their brains than do people with contusions (see Marklund et al., 2009). However, David Brody of Washington University in St. Louis, Missouri, notes that this study did not compare Aβ42 levels with those in uninjured brains. Therefore, it is possible that both types of injuries lead to lowered extracellular Aβ levels compared to normal brains, which would be consistent with other studies, Brody said (see, e.g., Magnoni and Brody, 2010).
A puzzling fact is that, although CTE is primarily a tauopathy, its dementia seems to be modulated by ApoE genotype (see Jordan et al., 1997). One possibility, Sam Gandy at Mount Sinai Medical Center in New York City told ARF, is that blows to the head set off transient Aβ deposition, but the brain’s ability to efficiently clear away these deposits after each insult depends on ApoE genotype. Each round of Aβ deposition may also trigger tau, Gandy suggested, with tau pathology persisting and becoming self-perpetuating, even after Aβ is cleared. This may be similar to what happens in Alzheimer’s disease, Gandy noted. One theory holds that “the reason Aβ-lowering therapies fail in the clinic is because subjects with mild AD have already passed into a self-sustaining tau-dependent phase,” Gandy wrote to ARF.
Does CTE also occur in soldiers and marines exposed to repeated blasts from improvised explosive devices? These explosions create pressure waves that flex through bones and compress the brain, so the injuries may not be equivalent to impact concussions. McKee has just begun to look at donated brains from veterans exposed to repeated blast damage. She said that, although it is too early to be certain, there do appear to be large overlaps between these brains and what she sees in athletes with multiple concussions. She expects there will be some differences as well. Football players may get around 1,000 sub-concussive hits per season from playing on the line, McKee said, and it is not yet clear how that corresponds to receiving shock waves from one or several explosions. It does appear that blasts have to be strong enough to cause disorientation in order to be damaging: A recent study showed that simply being near large weapon blasts, such as the firing of artillery shells, did not create any changes in CSF biomarkers (see Blennow et al., 2011). For the latest data on what blast exposure does to brains, read Part 4.—Madolyn Bowman Rogers.
Zetterberg H, Hietala MA, Jonsson M, Andreasen N, Styrud E, Karlsson I, Edman A, Popa C, Rasulzada A, Wahlund LO, Mehta PD, Rosengren L, Blennow K, Wallin A.
Neurochemical aftermath of amateur boxing.
Arch Neurol. 2006 Sep;63(9):1277-80.
PubMed.
Scientists are beginning to get a handle on what happens in the brains of athletes who suffer multiple concussions, but to date little research exists on how brains respond to the pressure waves from explosions. Elaine Peskind at the VA Puget Sound Health Care System, Seattle, and the University of Washington, Seattle, is gathering data on what kind of physical changes blast damage can cause in people. In a VA-funded project, she has been examining a group of 35 Iraq veterans who have each been exposed to multiple explosions. The soldiers are not cognitively impaired, but complain of memory problems, forgetfulness, and trouble concentrating. As a group, they perform about one-half to one standard deviation below age- and education-matched norms, Peskind said.
Peskind employs four neuroimaging techniques, two functional and two structural. All four techniques show brain changes in blast-exposed veterans compared to Iraq veterans without such exposure, Peskind said. Using positron emission tomography with the glucose analog fluorodeoxyglucose F18 (FDG-PET) to visualize the brain’s glucose metabolism, Peskind found lower metabolism in the posterior cingulate and parietal lobes in blast-exposed soldiers compared to Iraq-deployed controls, Peskind said. She noted that the pattern of changes is similar to that seen in early-stage mild cognitive impairment (MCI), although much less severe. Similarly, functional MRI imaging also showed MCI-like changes, with lowered activity in posterior cingulate cortex and parietal lobes. Both blast-exposed and non-blast-exposed veterans had hypometabolism in pons and cerebellum compared to civilian controls, as seen by FDG-PET (see Peskind et al., 2011).
Brains with mild TBI (top row) show a similar pattern of changes to MCI brains (bottom row) by PET scan.Image credit: Elaine Peskind
The structural techniques provided more detailed data on the nature of the changes and revealed axon damage. Diffusion tensor imaging, which measures the random movement of water in the brain, exposed flaws in the integrity of white-matter tracts, particularly in the cerebellum, Peskind said. Although FDG-PET showed lower metabolism in the cerebellum in all Iraq veterans, diffusion tensor imaging revealed worse cerebellar abnormalities in the blast-exposed veterans. The second structural technique, cross-relaxation imaging, gives an estimate of the health and density of myelin, as well as of changes in gray matter (see, e.g., Yarnykh and Yuan, 2004). Peskind said this technique revealed pronounced loss of structural integrity in both white and gray matter in blast-exposed veterans compared to unexposed colleagues.
The neuroimaging data still need to be replicated, Peskind cautioned. Even so, they raise potential concerns. Is repetitive blast trauma similar to repetitive impact trauma? If so, are veterans at risk for the neurodegenerative condition of chronic traumatic encephalopathy, seen in some athletes? Will veterans with these early brain changes have an increased risk of Alzheimer’s disease later in life? “Those are my concerns, but it’s certainly too early to draw any conclusions about it,” Peskind said.
Peskind hopes to follow these veterans, whose mean age is 34, over many years and monitor how their brains change. This data will be correlated with regular neuropsychological test results. Peskind’s group is also collecting cerebrospinal fluid (CSF) from the veterans to measure alterations in the levels of biomarkers such as Aβ42. They do not yet have enough CSF data to analyze, Peskind said. She is not doing any amyloid PET scanning, but Peskind points out that Aβ levels in CSF have been shown to fall before amyloid deposits become visible in the brain. Therefore, the researchers expect to catch early amyloid changes in the CSF. The veterans have also contributed DNA for genotyping several genes of interest: apolipoprotein E, the AD risk-modifying gene TOMM40, the tau gene MAPT, and brain-derived neurotrophic factor.
In the near term, cross-relaxation imaging shows good potential as a diagnostic, Peskind said, because the analysis is simple and the finding robust. In contrast, conventional MRI or CT scans are not useful to diagnose early TBI-related brain changes, points out David Brody of Washington University in St. Louis, Missouri. “Those techniques are just not sensitive enough to detect axonal injury,” Brody said.
Peskind’s data show global changes in brain structure and function, but what is happening at the cellular level in brains exposed to blasts? The shock wave of an explosion becomes a compression wave in the brain, subjecting cells to extreme pressure. In another VA-funded project, researchers led by Pamela VandeVord at the John D. Dingell VA Medical Center, Detroit, Michigan, and Wayne State University, Detroit, are developing models to answer this question (see VA story). VandeVord’s team uses a device called a barochamber to subject brain cell cultures to high pressure. The researchers have found elevated astrocyte reactivity in the hours following a pressure wave (see VandeVord et al., 2008 and Leung et al., 2008). Astrocytes respond by highly expressing genes involved in cell survival immediately after a blast, but minimal apoptosis. In contrast, neurons ramped up apoptotic genes in the first three days after a pressure wave, indicating these fragile cells were dying (Leung and VandeVord, 2009).
The Detroit researchers also expose rats to pressure waves by forcing a blast of air down a 22-foot-long metal tube, simulating what happens during an explosion. Initial experiments showed that this technique works to increase intracranial pressure, and that older rats with thicker skulls actually get hammered hardest, suggesting that the skull helps transmit pressure (see Leonardi et al., 2011). In ongoing work, the scientists will examine the rats with MRI, cognitive testing, and blood tests for biomarkers to dissect the effects of pressure on living brains. The researchers eventually hope to use these techniques to develop therapeutics to ameliorate the effects of blasts.
Such models may help to fill a gap in the field. McKee notes that one of the primary research needs is for better models of brain injury that accurately replicate human pathology. “We do not have a perfect model yet,” she said. For example, in one study of mild repetitive impact brain injury, only one out of 18 mice developed the expected neurofibrillary tangle pathology (see Yoshiyama et al., 2005).
Better animal models should help scientists find more effective treatments. To date, animal trials have translated poorly to people. For example, in mice, a statin called simvastatin reduced Aβ burden and improved cognition after TBI (see Abrahamson et al., 2009), implying it could reduce long-term AD risk, but human treatment trials of statins in AD so far have been unsuccessful. In the future, anti-tau therapies (which aren’t anywhere near regulatory approval yet) might show promise, McKee suggested, since tau pathology is prominent in CTE brains. Henrik Zetterberg at Sahlgrenska University Hospital in Molndal, Sweden, speculates that drugs that stimulate axon outgrowth and inhibit scar formation might be beneficial.
At the moment, “There is no standard of care other than symptomatic management,” Peskind said. McKee said much of the current focus for athletes is on prevention. By taking athletes out of action for a longer period of time after a mild brain injury, physicians hope to avoid some of the long-term complications from repeated trauma. The military is adopting the same procedures for wounded soldiers and marines, McKee said.
McKee sees some treatment potential in the finding that brain changes are already apparent in young athletes exposed to repetitive concussive injuries. “Hopefully, if we can get a handle on what causes those initial changes, we can prevent this disease from spreading into full-blown disease,” she said. All researchers interviewed for this story agreed that much more research is needed. Peskind summed it up: “We are in the infancy of studying a truly new and unique phenomenon.” For an overview of PTSD and dementia, check out Part 5.—Madolyn Bowman Rogers.
Stress and Trauma: The Puzzle of Post-traumatic Stress Disorder
The signature wound of modern war may be traumatic brain injury, but the picture is complicated by another invisible injury, that is, post-traumatic stress disorder. Developing as a reaction to a traumatic event, PTSD includes a cluster of symptoms ranging from nightmares, flashbacks, irritability, and hyperarousal, to emotional numbness and avoidance of places and objects that are reminders of the experience. Roger Pitman at Massachusetts General Hospital, Boston, told ARF that PTSD involves two kinds of brain changes: a conditioned fear reaction, in which certain cues incite anxiety, and sensitization to stimuli. For instance, people with PTSD startle easily. Research has also shown that people who develop PTSD may have a disturbance in their hypothalamic-pituitary system, Pitman said. Their increased number of glucocorticoid receptors corresponds to low levels of cortisol in the blood, predisposing a person to PTSD. In the big scheme of things, however, “We are still in the dark as to what the biological underpinnings of PTSD are,” said Norbert Schuff at the University of California in San Francisco.
The kinds of events that produce brain injuries are often traumatic, with the result that TBI and PTSD tend to go together. Elaine Peskind at the VA Puget Sound Health Care System and the University of Washington, Seattle, is conducting studies on a small group of veterans with TBI, as well as a small group of active-duty military with PTSD. She notes that three-fourths of these service members, all of whom were exposed to heavy combat, have both conditions. One study of returning military members concluded that PTSD and depression mediate many of the immediate poor health symptoms in soldiers with mild TBI (see Hoge et al., 2008), highlighting the importance of developing effective treatments for PTSD.
The long-term consequences of PTSD on the health of the brain remain an open question. Although TBI seems to have mechanistic links to dementia, the case to date is much weaker for PTSD. Only a couple of epidemiological studies have looked at the relationship. Both found provocative correlations. A large prospective study led by Kristine Yaffe at the San Francisco VA Medical Center and the University of California in San Francisco analyzed data from the VA’s national patient database on more than 180,000 veterans (see Yaffe et al., 2010). About 30 percent of the veterans had PTSD, and the researchers found that these veterans were more than twice as likely to develop dementia as those without PTSD over a period of about seven years. The results remained significant after adjusting for potential confounding factors such as TBI and depression. Another study found similar results, with veterans with PTSD having about twice the risk of dementia (see Qureshi et al., 2010).
What does this mean? Does PTSD influence the development of dementia, or are the two merely linked by some third factor? Some brain characteristics seen in people with PTSD, such as a smaller ventromedial prefrontal cortex, resemble features of AD, implying that the conditions could be related. Numerous studies have shown that people with PTSD have smaller hippocampi, also a hallmark of AD (see e.g., Bremner et al., 1995; Gurvits et al., 1996; Bremner et al., 1997; Hedges et al., 2003; Woodward et al., 2006). Nonetheless, Pitman urges caution in assuming that PTSD harms the brain. He points out that although PTSD may weaken some areas of the brain, other areas of the brain that mediate fear, such as the amygdala, are strengthened. “That may involve some adaptive brain plasticity that I am hesitant to call brain damage, although other people do call it brain damage,” Pitman said.
It is also possible that having a small hippocampus predisposes a person to PTSD. In other words, a small hippocampus may precede PTSD rather than following it. Pitman has conducted several studies on identical twins in which one twin had seen combat and the other had not. Some of the twins exposed to combat developed PTSD, and in agreement with other studies, these people had smaller hippocampi than combat veterans who did not get PTSD. What was interesting, though, was that the twins of the ones with PTSD also had smaller hippocampi, as well as lower cognitive performance and other subtle neurologic signs seen in people with PTSD, although these people had never seen combat and did not have the disorder (see Gilbertson et al., 2002; May et al., 2004; Pitman et al., 2006; Gurvits et al., 2006; Gilbertson et al., 2006; and Pitman, 2010). This suggests that these features are inherited risk factors for PTSD, rather than a result of a traumatic experience in war.
Along the same lines, one study claims that less intelligent people appear more likely to develop PTSD after a combat experience (see Macklin et al., 1998). Another study found no difference in hippocampal volume between veterans with and without PTSD, but saw that veterans who developed PTSD after their first exposure to a traumatic event had smaller hippocampi than those who developed the disorder after multiple traumas (see Yehuda et al., 2007). This, again, would support the idea that a smaller hippocampus is a risk factor for PTSD. Another study showed that among people with PTSD, reduced hippocampal activity was associated with more severe symptoms, implying that having a less active hippocampus can make a person more vulnerable to PTSD (see Astur et al., 2006).
Nevertheless, other studies do suggest mechanistic links between PTSD and the development of dementia. In both PTSD and AD, brain function is disturbed in the medial temporal lobe, hippocampus, and cingulate cortex, as seen by multiple forms of neuroimaging (see Tsolaki et al., 2009). Another imaging study concluded that the brains of people with PTSD showed numerous structural and physiological abnormalities in the frontal lobe and limbic regions, regions also affected by AD (see Schuff et al., 2011).
Hope, a painting by a Pakistani psychiatrist who treats PTSD. Image credit: Syed Ali Wasif via Wikimedia
A number of experiments on rodents have shown that prolonged stress can harm the hippocampus through the action of glucocorticoids (see, e.g., Sapolsky, 2000 and Dumas et al., 2010). High levels of homocysteine, a neurotoxic byproduct of cellular metabolism, have been seen in people with PTSD (see Levine et al., 2008 and Hasegawa, 2007). Since homocysteine is associated with higher dementia risk and shrinkage of the brain, this observation might provide a mechanism by which chronic stress could lead to dementia. Likewise, a recent imaging study led by Schuff showed that in people with PTSD, the hippocampus shrinks preferentially in the dentate gyrus, where new neurons are born in adulthood; this implies that “chronic stress suppresses neurogenesis and dendritic branching in these structures,” the paper concludes (see Wang et al., 2010).
“[The dentate gyrus] is one of the very few areas in the adult brain where there is regeneration of neurons,” Schuff said. “If this finding is replicated in other studies, then this gives a possibility for a pharmaceutical target to stimulate neurogenesis [that could] potentially help people who suffer from PTSD.”
Despite the link seen between PTSD and specific brain changes, “there are confounding third variables that would need to be controlled for,” Pitman cautions. “This work is all preliminary; it is suggestive. It deserves further pursuit.” Pitman observes that lower cognitive reserve, as measured by intelligence, might well predispose both to PTSD and to dementia-like brain changes, and is difficult to account for in studies. For her part, Elaine Peskind at the VA Puget Sound Health Care System, Seattle, and the University of Washington, Seattle, noted that “veterans who have PTSD have many health-related behavioral risks for dementia. [They are] more likely to smoke, more likely to be overweight, have hypertension, have sleep apnea.” Nevertheless, Yaffe points out that her study controlled for many of these factors and still saw an association between PTSD and dementia. See Part 6 for a discussion of how researchers might resolve this puzzle, and an overview of potential treatments.—Madolyn Bowman Rogers.
Stress and Trauma: Tackling Post-traumatic Stress Disorder
Despite evidence of a link between post-traumatic stress disorder (PTSD) and dementia, the picture remains hazy, and bringing it into focus will require animal studies and human neuroimaging. As detailed in Part 5, Kristine Yaffe, at the San Francisco VA Medical Center and the University of California in San Francisco, uncovered a connection between PTSD and dementia risk in a large prospective study. She will follow up on this work by comparing imaging and neuropsychologic profiles of people with PTSD to those of people with dementia, looking for mechanisms that connect the disorders.
Pathological scrutiny of PTSD brains may also yield clues. Ann McKee at the Bedford VA Medical Center, Massachusetts, who runs several brain banks, is hoping to establish a VA brain bank specific for PTSD. From the few PTSD brains she has examined to date, she believes there may be some overlaps between PTSD-related changes and those seen in other disorders such as chronic traumatic encephalopathy. One problem is that “PTSD at this point is a heterogeneous grab bag of different diseases,” McKee said. “We need to focus on strict criteria for PTSD.” However, Elaine Peskind at the VA Puget Sound, Seattle, Washington, noted that from a clinician’s point of view, PTSD symptoms are easily recognizable and measurable, making the diagnosis straight-forward.
Several researchers agree that longitudinal studies offer the best chance to establish if PTSD is a true risk factor for dementia. Such studies are difficult and expensive. Researchers would have to choose a population of people at high risk of experiencing traumatic events, and follow them for a long time to see who gets PTSD and who later develops dementia. A slightly easier job would be to use longitudinal studies to examine whether a small hippocampus, or some other structural feature, predisposes to PTSD, as some research suggests. Schuff said researchers could collaborate with the Department of Defense to perform brain scans on soldiers before and after deployment, and look for patterns in regard to which soldiers develop PTSD. Another option would be to study civilians in dangerous jobs, such as police officers or rescue workers.
If PTSD-related brain changes do increase the risk of dementia, then one of the most important questions to address is whether treating PTSD will lower that risk, Yaffe said. No one knows the answer, but promising clues exist. In a study of 244 Gulf War veterans, Schuff and colleagues found that a small hippocampus correlated with a current diagnosis of PTSD, but not with a past diagnosis (see Apfel et al., 2011). That implies either that a small hippocampus is a risk factor for failure to recover from the disorder, or, more hopefully, that the hippocampus may return to normal as PTSD symptoms subside.
Hope, a painting by a Pakistani psychiatrist who treats PTSD. Image credit: Syed Ali Wasif via Wikimedia
Unfortunately, effective treatments for PTSD are scarce. A 2007 report by the Institute of Medicine found evidence of efficacy for only one behavioral intervention, exposure-based therapy. The FDA has approved two medications to treat trauma, sertraline (Zoloft) and paroxetine (Paxil). All of these interventions work best for civilian trauma, however. No approved treatment has shown robust efficacy for combat veterans, whose PTSD often results from repeated traumas.
Several pharmaceutical agents are in clinical trials. One of the more exciting options is an FDA-approved anti-hypertensive medication called prazosin that acts to block the effects of adrenaline. Occasional side effects can include dizziness, fatigue, and nausea. In a small preliminary study, work by Murray Raskind, also at the VA Puget Sound, and Peskind has shown that this α-blocker can relieve nightmares and help active-duty soldiers with PTSD sleep better (see Calohan et al., 2010). Prazosin works even for veterans from the Vietnam War and World War II who have longstanding cases of PTSD, Peskind said (see Raskind et al., 2007; Raskind et al., 2003), and for civilians as well (see Taylor et al., 2008). The drug has also been used to calm agitation in people with AD (see Wang et al., 2009).
Raskind and Peskind are currently conducting a large 13-site VA cooperative study of prazosin for combat trauma. Raskind is also leading a Department of Defense study examining the effects of prazosin in active-duty military at Fort Lewis, Washington. Early results are promising, Peskind said. If the findings hold up, she believes prazosin may soon see widespread use in the VA and military for treating PTSD-related sleep disturbances. “We are very hopeful for being able to help this new generation of veterans,” Peskind said.
Intriguingly, the same medication has also shown promise for treating migraine headaches, which happen to be one of the most frequent symptoms of brain injury. When veterans were given prazosin after concussions, they reported fewer and milder headaches, slept better, and improved by four points on the Montreal Cognitive Assessment (see Ruff et al., 2009).
Better zzz’s may have far-reaching cognitive benefits. PTSD is often associated with nightmares and insomnia, and lack of sleep has numerous bad effects on the brain. For example, in animals, sleep deprivation blunts hippocampal-dependent learning and stops the birth of new neurons in this region (see Hairston et al., 2005). Schuff’s group found that in PTSD patients, the severity of insomnia correlated with volume loss in the dentate gyrus, suggesting that sleeplessness suppressed neurogenesis (see Neylan et al., 2010). “Sleep studies are a very strong component in PTSD [research],” Schuff said. Sleep loss has been tied to higher levels of Aβ in mouse models, suggesting a mechanism whereby chronic lack of sleep could predispose to AD (see ARF related news story on Kang et al., 2009).
Other PTSD drugs are in trials, but with mixed results so far. Roger Pitman at Massachusetts General Hospital, Boston, is excited by the use of the NMDA receptor agonist D-cycloserine, administered immediately following cognitive behavioral therapy, to help extinguish the fear response (see Davis et al., 2006 and Norberg et al., 2008). The drug has shown benefits in animal models (see Yamamoto et al., 2008), and for anxiety disorders (see, e.g., Ressler et al., 2004). However, in a previous small PTSD trial, the drug did not outperform placebo (see Heresco-Levy et al., 2002 and Internal Medicine News story).
Pitman is also studying the benefits of propanolol, a β-blocker used to treat hypertension and heart conditions, to prevent PTSD symptoms. When administered shortly after a trauma, it appears to lessen the incidence of PTSD (see Vaiva et al., 2003). Pitman and colleagues have also shown it can help reduce symptoms in established cases of PTSD when given immediately after reactivating traumatic memories (Brunet et al., 2008), and they are continuing to pursue this approach. So far, however, a randomized controlled trial of more than 500 people admitted to emergency rooms after a trauma found that propanolol was no better than placebo at preventing PTSD (see Stein et al., 2007).
No one has yet found a magic bullet. For both PTSD and traumatic brain injury, science has just begun venturing into largely unexplored land. Much more research will be needed to conquer this new frontier. Indeed, interested scientists will have a chance to show their data and learn the latest at a Keystone conference that is devoted to traumatic encephalopathies and will run jointly with another conference on ApoE and AD. Co-organized by Sam Gandy, Steven DeKosky, and Ann McKee, the meeting calls for abstracts this fall, so now is the time to put on thinking caps, run experiments, and crunch the data.—Madolyn Bowman Rogers.




Comments
No Available Comments
Make a Comment
To make a comment you must login or register.