$100M IDEAS: CMS Blesses Study to Evaluate Amyloid Scans in Clinical Practice
Quick Links
Two years after they first ran against a wall trying to get amyloid scans reimbursed by insurance, researchers now have their chance to prove the costly procedure is worth it. The Centers for Medicare & Medicaid Services (CMS) has approved the protocol for a four-year, $100 million study called Imaging Dementia—Evidence for Amyloid Scanning. IDEAS was spearheaded by Maria Carrillo of the Alzheimer’s Association and will be managed by the American College of Radiology (ACR) in Reston, Virginia. This massive study aims to examine how well amyloid imaging performs in clinics outside the small, rarefied world of clinical trials and tertiary academic care. IDEAS will measure whether getting a scan can affect the diagnosis, management, and future healthcare of people whose cognitive symptoms cannot be definitively attributed to a cause by clinical diagnosis alone. “More knowledge about clinical use of amyloid imaging is important not only for accurate diagnosis of Alzheimer’s, but also for the potential future use of a therapeutic agent,” Carrillo told Alzforum.
Under its coverage with evidence development (CED) mechanism, which requires research participation for reimbursement, the CMS will cover the cost of almost 18,500 patient scans from about 200 imaging centers around the country.
“We will learn a lot about how amyloid imaging functions in the real world,” said Gil Rabinovici, University of California, San Francisco, who is the study’s principal investigator. “The question of where it fits into our current diagnostic algorithm with the prevailing state of treatments is largely unanswered.”
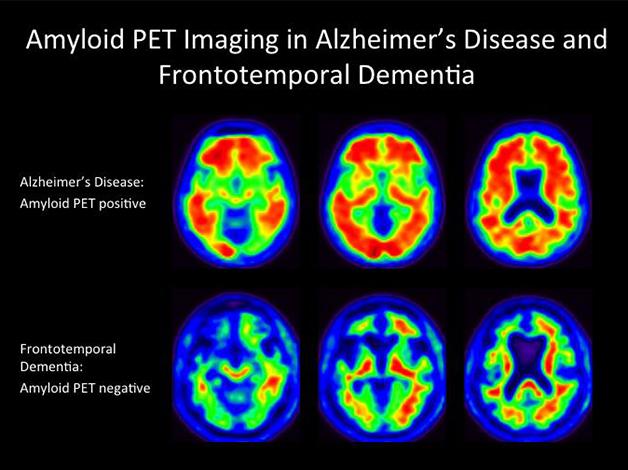
Worth the money? The IDEAS study aims to find out if amyloid PET scans change a patient’s diagnosis or disease management. [Image courtesy of Gil Rabinovici and William Jagust, prepared by Daniel Schonhaut.]
To date, CMS has refused to cover positron emission tomography (PET) scans that pick up evidence of amyloid, citing a paucity of evidence that they ultimately improve patient outcomes (Jan 2013 news; Jul 2013 news story). Several research groups have already characterized how an amyloid scan alters the diagnosis or treatment of patients, but these previous studies are single-center, smaller, and vary somewhat in how they were done (Ossenkoppele et al., 2013; Sánchez-Juan et al., 2014; Grundman, 2013; Zannas et al., 2014; Mitsis et al., 2014). IDEAS is a national study that might settle the question.
In its July 2013 decision, CMS offered hope that it could approve amyloid imaging for coverage in the future if the field generates more evidence. Within CED, CMS will reimburse for one amyloid scan for each cognitively impaired person taking part in a clinical trial, if that trial collects data about how the scan subsequently affected the patient’s health outcomes (Oct 2013 news). If enough data ultimately point to a patient benefit, CMS may decide to cover scans, at least for some patient subgroups.
This CED mechanism has been used successfully in other diseases. An example is the National Oncologic PET Registry (NOPR), which opened in 2006 and collected data on the clinical utility of fluorodeoxyglucose (FDG) PET in cancer. Before then, CMS had reimbursed for FDG-PET scans only for certain cancers. Under NOPR, CMS expanded coverage for more cancers on the condition that researchers send back to CMS information about how the scans affected treatment plans. After seven years, the registry had collected sufficient data showing changes in diagnosis and treatment plans for CMS to open coverage for FDG-PET to all types of cancer. This happened in June 2013, just before the amyloid PET case was turned down.
An amyloid PET scan costs several thousand dollars. The CMS now wants scientists to show whether amyloid PET imaging pulls its weight in the clinic. The IDEAS study is designed to do that. To gain approval for the study, the researchers first had to reassure the CMS that amyloid scans would be limited to defined circumstances in which they would be clinically useful, and not given to anyone who complained to their primary care physician about memory problems. In accordance with criteria for appropriate use published two years ago (see Jan 2013 news; Johnson et al., 2013), Rabinovici and colleagues specified that the only people who can enroll must meet formal diagnostic guidelines for mild cognitive impairment (MCI) or dementia, and an evaluating dementia expert must be uncertain whether the cognitive symptoms are caused by Alzheimer’s disease or something else. Rabinovici emphasized that this study is not for cognitively normal people or for people whose Alzheimer’s diagnosis is straightforward. “The referring dementia expert must have spent significant time with the patient, and performed a complete assessment to arrive at a diagnosis of MCI or dementia with uncertain etiology,” Rabinovici said.
Referring clinicians have to meet certain criteria, as well. Physicians who are trained and board-certified in neurology, psychiatry, or geriatric medicine, and who spend at least a quarter of their time evaluating adults with cognitive impairment, will be eligible to prescribe scans in this study.
From 2016 to 2017, IDEAS aims to enroll 18,488 Medicare beneficiaries aged 65 and older. Before a patient gets a scan, the referring clinician will fill out a case report form with the diagnosis and the intended treatment plan. Patients will then undergo amyloid imaging with whichever one of the three FDA-approved tracers—florbetapir, flutemetamol, or florbetaben—is being used at their local center. Three months after the referral, the clinician will submit a second, updated report that details the new diagnosis and treatment plan incorporating results of the amyloid PET scan. These electronic forms will go to the ACR cloud-computing center, which hosted data from NOPR.
The first aim of the IDEAS protocol calls for researchers to determine whether and how the scan result affects short-term patient management—diagnosis, drug treatment, additional testing, safety counseling, and planning for the future. The primary objective is to see if the scans lead to a change between intended and actual plans in 30 percent of cases. A secondary objective is to track whether scans reduce unnecessary diagnostic procedures and treatments.
The second aim is to look at the following year of Medicare claims. The researchers want to know if having a scan reduces subsequent hospitalizations and emergency-room visits compared with a control group of unscanned people matched for age, cognitive impairment, and comorbidities. Altogether, IDEAS is a 4-year study.
IDEAS is a big undertaking. Its recruitment goal is ambitious. Even so, Rabinovici anticipates wide participation. The workload for clinicians is light, and he believes the opportunity to bring scans to the patients who need them most will appeal to doctors. “As a clinician, I see multiple cases that would meet the criteria each week,” said Rabinovici. Physicians will receive a modest stipend for the time it takes to fill out the case-report forms. To recruit dementia experts, Rabinovici and others will advertise via news media and professional organizations such as the American Society of Neuroradiology and the American Academy of Neurology. They will also send information to distribution lists related to nuclear medicine and dementia, and to networks of imaging sites that have taken part in clinical trials for cognitively impaired people.
A group of experts in amyloid imaging or dementia and others with experience conducting studies of this scope designed IDEAS and will analyze its results. Besides Rabinovici, they are Rachel Whitmer, a dementia epidemiologist at Kaiser Permanente Division of Research, Oakland, California; Barry Siegel of Washington University, St. Louis; and Bruce Hillner from Virginia Commonwealth University, Richmond, who jointly led NOPR. Constantine Gatsonis of Brown University in Providence, Rhode Island, led statistical analyses for NOPR and will do the same for IDEAS.
Now that CMS has approved the study, the researchers are entering a development period and then hope to start enrolling in January 2016. CMS has agreed to pay for the scans and their interpretation, which the researchers estimate will cost about $80 million. “This study will bring an additional $100 million to the field, much of it from CMS, which has not contributed in so large a fashion before,” Carrillo said. In addition, almost $20 million is budgeted for research infrastructure, investigator time, case-report forms, and databases; this will come from a mix of philanthropic and industry funds. Carrillo said she has yet to nail down who will contribute how much, but she is in talks with stakeholders, and the association will pitch in some funds, too. Of the three tracer manufacturers—GE Healthcare, Piramal Imaging, and Avid/Lilly—the former two confirmed to Alzforum that they plan to contribute, and the latter wrote that it is currently evaluating whether to fund.
Meanwhile, the tracer companies are gearing up to distribute their ligands more widely. Many of the participating imaging centers have yet to be identified and enrolled. After that, companies will look to expand their delivery and fill in gaps. Avid/Lilly currently manufactures florbetapir at about 30 sites, GE Healthcare makes flutemetamol at seven, and Piramal makes florbetaben at 11. They each distribute to pharmacies from there.
“This is a very important study, and one of the key activities we are performing in the U.S. right now,” said Andrew Stephens, chief medical officer of Piramal, adding, “The ability for CMS to get behind this study shows that they are interested and involved, and this will hopefully lead to reimbursement in the future.” Ben Newton, director of PET neurology at GE Healthcare, agreed. “If we can show clinical impact, that might translate into a decision to reimburse for PET amyloid imaging. That would have a huge impact on the growing dementia population in the United States,” he said. It would also help the companies’ bottom line.
Researchers from around the country sounded excited about the green light for this long-anticipated study. For example, Hillner said that the hope is for this one study, if positive, to be enough to persuade the CMS to come around. Stephen Salloway of Brown University was part of the committee that helped plan and organize the study and will participate as a referring clinician. “IDEAS opens a new door for studying the benefit of amyloid PET in patients with possible Alzheimer’s disease,” Salloway told Alzforum. He said his motivation is to improve care for his patients, who will be better able to plan when they get a more accurate diagnosis.
Why do patients want to know? “The underlying principle is that if you get a specific diagnosis early, you may be able to prevent a bad outcome,” Rabinovici told Alzforum. For instance, if you knew your mother had MCI due to AD, you might make sure she no longer takes her prescribed insulin or warfarin by herself and potentially ends up in the emergency room with low blood sugar or a hemorrhage. You might take less action if the doctor did not explain what was going on because he was uncertain. “In those scenarios, our system of care is reactive,” said Rabinovici. “We wait until a health emergency has occurred. Being proactive and trying to prevent these bad outcomes is the motivation behind this study.” With a definitive diagnosis, patients can receive better counseling about safety, advance directives, driving, and taking medication.
Other participants will receive negative results that prompt their physicians to search for potentially treatable causes for the cognitive impairment, such as a sleep disorder or depression. “Without the scan it might have been attributed to AD and no further workup would be done,” Rabinovici told Alzforum. Participants with a positive scan could go on to participate in clinical trials if they wished, he pointed out.
So far the IDEAS study is the largest to be CMS-approved under the CED mechanism, but it is not the only one. Two smaller studies are ongoing. Led by Daniel Silverman at the University of California, Los Angeles, the Molecular Cerebral Imaging in Incipient Dementia (MCI-ID) II will examine how PET amyloid imaging, FDG-PET, or a combination, affect the future cognitive decline, diagnosis, management, and healthcare expenses of 1,500 patients with MCI. MCI-ID is set to run until 2020. In addition, the Alzheimer's Prevention Through Exercise (APEx) study will assess the ability of a year of aerobic exercise to reduce amyloid burden and cognitive decline in 100 non-demented people who have evidence of amyloid in the brain. Jeffrey Burns, University of Kansas, is leading that study, which runs until 2018.—Gwyneth Dickey Zakaib
References
News Citations
- Not So Fast: Amyloid PET Needs More Data Before Insurance Pays
- Coverage Denial For Amyloid Scans Riles Alzheimer’s Community
- Miami: Longitudinal Amyloid PET Data Start Converging
- HAI—Amyloid Imaging in the Clinic: New Guidelines and Data
Paper Citations
- Ossenkoppele R, Prins ND, Pijnenburg YA, Lemstra AW, van der Flier WM, Adriaanse SF, Windhorst AD, Handels RL, Wolfs CA, Aalten P, Verhey FR, Verbeek MM, van Buchem MA, Hoekstra OS, Lammertsma AA, Scheltens P, van Berckel BN. Impact of molecular imaging on the diagnostic process in a memory clinic. Alzheimers Dement. 2012 Nov 16; PubMed.
- Sánchez-Juan P, Ghosh PM, Hagen J, Gesierich B, Henry M, Grinberg LT, O'Neil JP, Janabi M, Huang EJ, Trojanowski JQ, Vinters HV, Gorno-Tempini M, Seeley WW, Boxer AL, Rosen HJ, Kramer JH, Miller BL, Jagust WJ, Rabinovici GD. Practical utility of amyloid and FDG-PET in an academic dementia center. Neurology. 2014 Jan 21;82(3):230-8. Epub 2013 Dec 18 PubMed.
- Grundman M, Pontecorvo MJ, Salloway SP, Doraiswamy PM, Fleisher AS, Sadowsky CH, Nair AK, Siderowf A, Lu M, Arora AK, Agbulos A, Flitter ML, Krautkramer MJ, Sarsour K, Skovronsky DM, Mintun MA, . Potential impact of amyloid imaging on diagnosis and intended management in patients with progressive cognitive decline. Alzheimer Dis Assoc Disord. 2013 Jan;27(1):4-15. PubMed.
- Zannas AS, Doraiswamy PM, Shpanskaya KS, Murphy KR, Petrella JR, Burke JR, Wong TZ. Impact of ¹⁸F-florbetapir PET imaging of β-amyloid neuritic plaque density on clinical decision-making. Neurocase. 2014 Aug;20(4):466-73. Epub 2013 May 14 PubMed.
- Mitsis EM, Bender HA, Kostakoglu L, Machac J, Martin J, Woehr JL, Sewell MC, Aloysi A, Goldstein MA, Li C, Sano M, Gandy S. A consecutive case series experience with [18 F] florbetapir PET imaging in an urban dementia center: impact on quality of life, decision making, and disposition. Mol Neurodegener. 2014 Feb 3;9:10. PubMed.
- Johnson KA, Minoshima S, Bohnen NI, Donohoe KJ, Foster NL, Herscovitch P, Karlawish JH, Rowe CC, Hedrick S, Pappas V, Carrillo MC, Hartley DM. Update on appropriate use criteria for amyloid PET imaging: dementia experts, mild cognitive impairment, and education. J Nucl Med. 2013 Jul;54(7):1011-3. PubMed.
External Citations
Further Reading
Papers
- Laforce R Jr, Rabinovici GD. Amyloid imaging in atypical dementia. CMAJ. 2014 Jun 10;186(9):695. Epub 2014 Jan 20 PubMed.
News
External Links
Annotate
To make an annotation you must Login or Register.
Comments
Alzheimer Center Amsterdam; Head EQT Life Sciences Dementia Fund
IDEAS is a much-needed study. The main outcome from the perspective of third payers will be health economics. It is likely that with the current pricing of amyloid PET scans and the absence of any specific, approved, anti-amyloid-directed therapy, the cost at present will not outweigh the benefits.
This may be very different from CSF, for instance, given the much lower pricing. As such, it is a pity that there is no direct comparison made in IDEAS between LP and PET, in a substudy, for instance. That may have to do with the continued reluctance on the part of physicians in the U.S. to perform lumbar punctures. In Europe, the situation may different for some countries, where LP is added to the standard routine practice and LP plus essays are at least partly reimbursed (Molinuevo et al., 2014). Given the considerable difference in price level of CSF assessment vs. PET in Europe, the economic case for LP is easier to make, not even taking into account that CSF provides more information than just amyloid status (Kvartsberg et al., 2014).
References:
Molinuevo JL, Blennow K, Dubois B, Engelborghs S, Lewczuk P, Perret-Liaudet A, Teunissen CE, Parnetti L. The clinical use of cerebrospinal fluid biomarker testing for Alzheimer's disease diagnosis: a consensus paper from the Alzheimer's Biomarkers Standardization Initiative. Alzheimers Dement. 2014 Nov;10(6):808-17. Epub 2014 Aug 20 PubMed.
Kvartsberg H, Duits FH, Ingelsson M, Andreasen N, Öhrfelt A, Andersson K, Brinkmalm G, Lannfelt L, Minthon L, Hansson O, Andreasson U, Teunissen CE, Scheltens P, Van der Flier WM, Zetterberg H, Portelius E, Blennow K. Cerebrospinal fluid levels of the synaptic protein neurogranin correlates with cognitive decline in prodromal Alzheimer's disease. Alzheimers Dement. 2015 Oct;11(10):1180-90. Epub 2014 Dec 19 PubMed.
Make a Comment
To make a comment you must login or register.