At Age 8, DIAN Is Churning Out Data and Growing into a Movement
Quick Links
Part 1 of a five-part report.
At age 8, DIAN has grown up. In 2008, when the Dominantly Inherited Alzheimer’s Network formally began to study autosomal-dominant AD, the notion of assembling globally dispersed families afflicted with this rare form of AD into a standing research platform seemed radical to observers. In theory, the idea of characterizing the preclinical course of their disease, and using that knowledge to conduct prevention trials, was enticing. But could it really be done? In 2016, at the Alzheimer’s Disease International Conference July 22-28 in Toronto, the answer to that was plainly on display.
DIAN’s first therapeutic trial, testing two investigational antibodies, is fully enrolled and expecting a preliminary biomarker readout this winter. The second stage of the trial is slated to start enrolling next spring, and plans for a primary prevention trial—in people in their 20s—are taking shape. Meanwhile, the observational DIAN study has logged some 1,500 participant visits to date. It is beginning to churn out the longitudinal data across all observed markers of disease that will put the progression rates researchers had estimated based on cross-sectional data on a more definitive footing. From this in-person serial data, a disease progression model is being built to undergird intervention trials.
A New Generation’s Fighting Spirit.
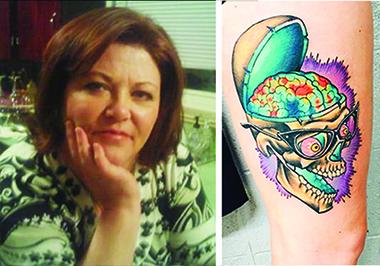
On February 25, 2015, Lori DeMoe McIntyre died of Alzheimer’s disease at age 56, after participating in DIAN research for nearly eight years. Her daughter Jessica McIntyre memorialized her mom with a large tattoo of her amyloid PiB PET scan. The younger McIntyre and one of her sisters participate in DIAN and DIAN-TU. [Courtesy of Jessica McIntyre, art by Joey Borger, Certified Customs, Denver, Colorado.]
DIAN scientists have begun an ambitious effort to compare their data to comparable data sets in late-onset AD (LOAD). It is their attempt to settle—for regulators and the field at large—the long-standing debate about how similar, or different, early onset and late-onset Alzheimer’s disease truly are. The DIAN network itself is expanding not only the number of its member sites and countries, but also the sample, resource, and data collections that it offers to outside scientists for independent analyses. “DIAN is gathering tremendous momentum,” said Nick Fox of University College London, an original DIAN site, adding, “This is exciting to see, after years of small studies that had too little power to answer questions and deliver subjects to trial.”
The network’s families are meeting in gatherings that increasingly feel like reunions. Relatives are gaining confidence in sharing their experiences. They inject hope, humor, even spunk into serious conversations about intensely painful topics. Increasingly, their young adult members are joining, and getting to know each other. Updates on all of these fronts came in the form of a daylong meeting that drew 118 family members and as many scientists and other stakeholders, a meeting of DIAN’s steering committee with family representatives present, as well as separate meetings for international sites wishing to join, existing sites prepping for the next therapy trial, a featured research session, and a slew of individual talks and posters throughout the AAIC conference itself. Below are selected highlights.
First, the treatment trial. It is being run by the DIAN Trials Unit, a spin-off of the original observational study, DIAN-TU and DIAN-Obs for short. This four-year trial is the first intervention study designed solely for autosomal-dominant AD. Last December, it met its enrollment target of 210 people who range between 15 years before and 10 years after their particular mutation’s expected age of clinical onset. The trial compares the immunotherapies solanezumab and gantenerumab to a pooled placebo group, and it does so without requiring that participants find out their mutation status.
Unlike early stage trials in LOAD, which grapple with screen failure rates of up to 80 percent, only 19 percent of people who tried to join the DIAN trial ran afoul of an inclusion or exclusion criterion, Randy Bateman of Washington University, St. Louis, said at AAIC. About half the trial participants previously had been in the DIAN observational study, 15 percent entered directly via clinical sites, and 38 percent found the trial by way of the DIAN Expanded Registry.
The ideal scenario is for participants to join the observational study for a while so researchers can collect some data on their biomarker trajectories, and then to enter an intervention trial that is suitable for them. At the end of the trial, participants can return to the observational cohort or join another trial until a drug is found that works, said Bateman. The whole public-private enterprise of DIAN is a continually operating research and trials machine that does not waste data by disbanding at the end of a given drug study. To make this possible, DIAN and DIAN-TU take harmonized assessments on many markers, such that run-in data from the observational study, and placebo data from a trial, can feed into a disease progression model the scientists have built.
The DIAN participants understand the network’s mission well. In a field where dropout rates of 30 percent are routine, 2 percent per year have dropped out of the current DIAN-TU treatment trial, Bateman said. Another handful had to leave per the trial’s protocol, because they decided midway through to find out their genetic status and discovered they had not inherited the family’s Alzheimer’s disease mutation. Their departures will not reduce the trial’s power, because non-carriers are included to help keep the overall group blinded to everyone’s mutation status, not to contribute to the actual drug evaluation data. Importantly, the trial’s completion rate for its intensive battery of clinical, cognitive, fluid and imaging measures is nearly 100 percent. “This is unheard of in AD clinical trials, and it speaks to the commitment of family members and centers,” Bateman said. For a clinical trial as small as this, a near-perfect completion rate greatly helps its statistical power.
The second stage of the DIAN-TU trial, dubbed NexGen, is widely expected to add a third drug in early 2017. Despite ample speculation about which one it will be, DIAN investigators at AAIC kept mum on the subject. They readily talked about the new features of the NexGen stage of the trial, though. It will also treat people for four years, with a biomarker readout at year one and potential interim cognitive readouts at years two and three. NexGen can adjust the administered dose up to achieve maximal effect. The point of doing this is to avoid a scenario that has happened before in AD, whereby a trial proceeds to its end only for scientists to discover the dose had been too low all along. These trials are long, and the families keep saying their situation is too urgent for conventional fixed-dose designs. NexGen will pool placebo data from the first two drug arms in order to further increase power and keep the fraction of participants who don’t get drug low, at 25 percent. That is being done because the prospect of being on placebo for four years is perhaps the families’ top complaint. The new trial will enable cognitive testing at home in an effort to improve cognitive estimates and reduce the burden on its middle-aged participants, who are working and raising children.
Most importantly, perhaps, NexGen uses an ADAD-specific disease progression model WashU scientists have been building with longitudinal data from the observational study. To date, DIAN-Obs has tracked in-person change on cognition and biomarkers for a period of up to six years. For their research, DIAN scientists anchor where along the trajectory to AD symptoms each DIAN participant is, based not on their biological age but on how far away they are from their specific mutation’s mean age at symptom onset. This expected year of onset (EYO) is calculated from the mean age at onset of all known carriers of that particular mutation, not only the carrier’s own family. In essence, plotting a given participant’s cognitive, clinical, and biomarker trajectories relative to their EYO tightens up the variance of the raw data.
Built from this data, the disease progression model essentially lays out a quantitative path for the disease. This then allows scientists to predict what a drug effect of, say 30, 50, or 70 percent should look like in terms of cognition, the primary outcome measure for these trials. “Using data from DIAN-Obs in this way gives our trials a substantial increase in power,” Bateman said, adding that regulators have been supportive of evaluating both the EYO concept and the use of the disease progression model for the trial. This so-called NexGen trial received funding from the Alzheimer’s Association and has a grant submission pending at the NIA.
With one trial halfway done and one about to start, Eric McDade at WashU has set his sights on the horizon. That horizon is primary prevention. Such a trial would treat people in hopes that they never develop amyloid deposition, or the subsequent pathophysiology of Alzheimer’s disease, in the first place. Essentially, it would mean giving investigational Alzheimer’s medications for many years to some college-age people and others in their 20s to early 30s. Why is that not an outlandish prospect anymore? For several reasons, McDade said.
Number one, the targets are in hand. Longitudinal data analyses from the DIAN observational cohort indicate that the cognitive tests used in DIAN pick up a subtle decline in cognition starting as early as 15 years before a person’s EYO. That is a big change from what was known before. It opens up an earlier window for therapeutic intervention, McDade said. Scientists are also gaining a more robust handle on the trajectories by which preclinical biomarkers diverge between mutation carriers and non-carriers prior to 15 years EYO, and on the order by which biomarkers change. These trajectories essentially become targets for intervention, McDade believes.
Number two, the participants may be there, too. Even as 89 people left DIAN-Obs to enter the solanezumab/gantenerumab trial, 289 are currently in DIAN-Obs and are hoping for a trial. In a survey Joshua Grill of the University of California, Irvine, conducted among DIAN participants, 90 percent said they would stay in trials that last longer than five years, and a majority said people younger than 15 years before their EYO should be offered a trial. “The families want trials for their young. It is a very important point for them,” McDade said.
Anecdotally, the second DIAN family meeting held in conjunction with AAIC featured a substantial number of young adults who are starting to get to know each other. One young man spoke about traveling from his home in Canada to Boston, and using his love of U.S. history as a balm to overcome the apprehensions of a first DIAN study visit. Another young man articulated a widely felt sentiment when he described how hearing his mom utter certain stock phrases long after her cognition had failed made him question the veracity of his childhood and adolescent memories of her saying those phrases in moments he had held dear. A 20-year-old woman, whose symptomatic father spoke of writing everything down at work so he could continue to provide for his family, was there the second year in a row. An 18-year-old man, who also has been watching his father decline, told this reporter he would “absolutely” enter a primary prevention trial if there was one for him. McDade received a grant from the GHR Foundation to prepare for such a trial.
For an AAIC news update on DIAN-Obs, and other data garnered on dominantly inherited Alzheimer’s disease, see Part 2 through Part 5 of this series as each is posted this week.—Gabrielle Strobel
References
Therapeutics Citations
News Citations
External Citations
Further Reading
No Available Further Reading
Annotate
To make an annotation you must Login or Register.
Comments
No Available Comments
Make a Comment
To make a comment you must login or register.